
We make a living by what we get, but we make a life by what we give.
Winston Churchill
Relationship Thesaurus Entry: Mentor and Protégé
From Writers Helping Writers:
Successful stories are driven by authentic and interesting characters, so it’s important to craft them carefully. But characters don’t usually exist in a vacuum; throughout the course of your story, they’ll live, work, play, and fight with other cast members. Some of those relationships are positive and supportive, pushing the protagonist to positive growth and helping them achieve their goals. Other relationships do exactly the opposite—derailing your character’s confidence and self-worth—or they cause friction and conflict that leads to fallout and disruption. Many relationships hover somewhere in the middle. A balanced story will require a mix of these dynamics.
. . . .
Mentor and Protégé
Description: This relationship consists of an experienced mentor who has achieved a measure of expertise in a given area and a protégé dedicated to learning from them and following in their footsteps. While a relationship can initially be established with this purpose in mind, the mentor/protégé dynamic typically grows out of an existing relationship (teacher/student, coach/athlete, boss/employee). The interactions between the two parties will differ based on many factors and may change over time.
Relationship Dynamics:
Below are a wide range of dynamics that may accompany this relationship. Use the ideas that suit your story and work best for your characters to bring about and/or resolve the necessary conflict.
A mentor eagerly sharing the fruits of their knowledge with the protégé
A mentor taking a personal interest in their protégé
A mentor actively creating growth opportunities for the protégé—taking them to meetings and introducing them to other influencers, etc.
A mentor being open to learning from the protégé
A mentor jealously keeping the protégé to himself
A mentor who doesn’t want the protégé to move on (seeing him or her as a valuable resource rather than someone with potential) and doesn’t do what is needed to grow them
A mentor viewing the protégé as an underling to do their busy work
A brilliant mentor who isn’t necessarily good at teaching or dealing with people
A mento taking the protégé’s lack of interest or ability personally
A protégé recognizing what the mentor can provide and soaking up everything they can
A protégé seeing the relationship not just as one that benefits him but also looking for ways he can help the mentor
A protégé catching up with their mentor and growing past him or her
A protégé taking the opportunity seriously, being responsible and showing gratitude
An overconfident protégé not being open to feedback from the mentor
A protégé seeking constant instruction, feedback, and affirmation from the mentor
A reluctant protégé only putting in partial effort
An eager protégé being distracted by personal problems and not giving the relationship their all
An unwilling protégé being pushed into the relationship (by parents, a court order, etc.), resulting in apathy or resentment
Conflicting Desires that Can Impair the Relationship
The mentor wanting something different for the protégé than the protégé wants
Either party wanting more time, energy, or personal attention than the other is willing or able to give
The mentor wanting to teach a protégé who is in the relationship for subversive reasons (to gain information for someone else, to set the mentor up for failure, to humiliate them, etc.)
A protégé wanting to learn from a mentor who wants to control and subdue
The protégé wanting to be taught and mentored while the mentor wants a lackey
Both parties wanting to be “top dog” in the relationship
Link to the rest at Writers Helping Writers
A history of free expression charts its seesawing progress
From The Economist:
A global firestorm erupted in 2005 after the publication in a Danish newspaper of 12 provocative cartoons of the Prophet Muhammad. Jacob Mchangama, a Dane and then a young lawyer, was dismayed. In the Muslim world he watched states that rarely allowed protest of any kind encourage violent demonstrations. Those governments also redoubled their diplomatic efforts to define “defamation of religions” as a human-rights violation that should be banned everywhere.
He found the response elsewhere even more alarming. Respectable people across the Western world blamed the cartoonist and his editors, not the repressive forces that drove the newspaper staff into hiding. This was not what Mr Mchangama, the product of a confidently secular Nordic democracy, had expected.
As his new book recalls, free expression was suffering setbacks on other fronts, too. In the late 1990s, when he was a student, the internet presaged a glorious era of liberty for people who otherwise lacked money or power to speak and organise. The victory in 2008 of Barack Obama, an erstwhile outsider, marked a high point of those expectations. Even then, though, digital freedom was already in retreat. Authoritarian regimes proved adept at exploiting and policing social media for their own malign ends. Western governments were often heavy-handed in their regulation of extremist discourse. And the gigantic power wielded by a few tech companies was troubling, regardless of how they used it.
All this led Mr Mchangama (whose paternal forebears came from the Comoro Islands) to apply his legal mind to supporting intellectual liberty: by podcasting and founding a think-tank, and by studying free expression’s fluctuating fortunes over the past 25 centuries. His conclusions, presented in a crisp and confident march through Western history, are sobering.
His view that freedom of speech is under threat from many directions—and, politically, from both right and left—is not original. More distinctive is his determination to show the ebb and flow of liberty as a dynamic process, under way at least since the era of ancient Greece. Accordingly, stringent repression of thought and speech becomes self-defeating and stimulates brave opponents. But great bursts of freedom also prove finite.
For example, the intellectual energy unleashed by the printing press and the Protestant Reformation was dissipated in waves of sectarian wars and mutual persecution. After the shock of the American and French revolutions, and the rise of Napoleon Bonaparte, Britain’s establishment became severely repressive in the early 19th century. But a countervailing movement of liberal thought and debate, carried along by technological and social change, proved more powerful.
Yet that trend, too, had its limits and its hypocrisies. John Stuart Mill was a brilliant Victorian advocate of intellectual freedom, but he participated in, and defended, the colonial administration of India. And as Britain became more open and tolerant at home, it curbed liberty of expression in its overseas possessions, especially amid the rise of independence movements.
The effects of colonial repression continued to be felt long after colonialism ended, as the book shows. Laws dating from the British Empire have been used to stifle dissent in modern India, and recently in Hong Kong. Measures that strangle freedom can easily outlive the conditions that engendered them—as, luckily, can laws and constitutions that entrench liberty. In America, where the possibility of frank, productive debate seems threatened by cultural warfare, the constitution’s First Amendment sets a limit on any faction’s ability to muzzle its opponents.
Link to the rest at The Economist
Stalin’s Library
From The Wall Street Journal:
Edward Gibbon sits proudly upon my bookshelf. A set of volumes that I own, neatly stacked, comprises his “History of the Decline and Fall of the Roman Empire.” What do you make of me because it is there? The set might indicate that I am a classicist, a scholar. It could signal my ambition—or my vanity. Perhaps it marks me as an anachronism: In this impatient, up-to-the-second moment, I display something written almost 250 years ago about a subject that is itself far older. While you form your judgment, let me divulge a secret. I have not read to the end of the famous series. Somewhere between Julian’s residence at Antioch and the revolt of Procopius, I lost the thread and laid Gibbon aside.
A famous reader who is the subject of a fascinating new study would have sniffed me out. Joseph Stalin went into the libraries of Communist Party officials to see if their books had truly been read or merely served to decorate the room. Stalin prized his own books and used bookmarks rather than dog-earing a page, good man. Yet his literary hygiene was not above reproach. One lender complained that Stalin smudged the pages of books with greasy fingerprints. As the party’s general secretary, he sometimes disregarded due dates. After he died in 1953, many of the volumes he had borrowed from the Lenin Library were quietly returned, the late fees unpaid.
Why should this matter of a cruel tyrant responsible for the deaths of millions of people? Geoffrey Roberts, a professor emeritus of history at University College Cork in Ireland, notes in “Stalin’s Library: A Dictator and His Books” that Stalin kept no diary and wrote no memoirs. Therefore his personal library, which he carefully maintained and treasured, offers a unique window into his thoughts. “Through an examination of these books,” Mr. Roberts writes, “it is possible to build a composite, nuanced picture of the reading life of the twentieth century’s most self-consciously intellectual dictator.”
That is a complex claim. Mr. Roberts doesn’t assert that Stalin’s books or the marks he made in them hold the key to his psyche. And the word “intellectual” will raise an eyebrow—the man was as coarse as smashed rocks—although “self-consciously” is an essential qualifier. Stalin wasn’t a gifted rhetorician or purveyor of original ideas like his contemporaries Lenin and Trotsky, yet he lived in their highbrow shadow. Mr. Roberts writes that “complexity, depth and subtlety” were not his strengths. Instead, his “intellectual hallmark was that of a brilliant simplifier, clarifier and popularizer.” The American diplomat Averell Harriman observed that Stalin possessed “an enormous ability to absorb detail.” He came to meetings “extremely well-informed.”
. . . .
Books were his secret weapon. During World War II, Stalin read widely on topics like military strategy, artillery and field tactics. At other times, he devoured volumes on history and Marxism. He had always been a reader, Mr. Roberts says. As a boy, Stalin was a bookworm; in the seminary, he was censured for reading forbidden novels on the chapel stairs. His daughter, Svetlana, said that in his Kremlin apartment there was scarcely room for art on the walls because they were lined with encyclopedias, textbooks and pamphlets, many well-thumbed. Stalin often asked others what they were reading and was known to interrupt meetings by taking down a volume of Lenin’s to “have a look at what Vladimir Ilyich has to say.”
At the time of his death, Mr. Roberts estimates, Stalin’s personal library ran to approximately 25,000 books, pamphlets and periodicals. Roughly 11,000 were classics of Russian and world literature by authors like Pushkin, Gogol, Tolstoy, Chekhov, Hugo and Shakespeare. The remainder were nonfiction titles in Marxism, history, economics and other fields. Lenin was far and away the most represented author, at nearly 250 publications—there were also scores of works by Bukharin, Trotsky and Engels. Stalin had his own ex-libris stamp and classification system. The centerpiece of his Moscow residence was its library, although he preferred to store his collection off-site and have an assistant bring him reading material upon request.
Link to the rest at The Wall Street Journal (PG apologizes for the paywall, but hasn’t figured out a way around it.)
How Emotionally Intelligent People Use the ‘Emotional Postmortem’ to Control Their Emotions and Improve Their Relationships
PG thought this item might be useful for character-building.
From Inc.:
“Oh, boy. This time I messed up.”
That’s what I was thinking when some years ago, I let my emotions get the best of me. I believed a colleague had stolen something of mine. Not literally; I thought he stole an idea. At least, that’s how I felt.
I knew the way I should handle it. I knew I should approach him calmly, state my concern without any type of accusation, and give him the chance to explain the situation.
But that’s not what I did.
Instead, I went in like a ticking time bomb, asking emotionally charged questions before …
I went off.
In the end, it turned out to be a huge misunderstanding. I felt horrible, because the colleague was a nice guy, and up until that moment we had a pretty good relationship. Of course, I apologized profusely, and he said it was OK and we’d consider it water under the bridge.
But to this day, every time I think of that moment, I cringe.
If you’ve ever had a moment like this one, maybe you can relate. In emotional intelligence terms, we refer to this as an emotional hijack.
In an emotional hijack, a small part of your brain known as the amygdala, which serves as a type of emotional processor, “hijacks” your brain and causes you to react without thinking. In my case, some built-up tension and various other factors caused me to see a situation unclearly, jump to conclusions, and hurl harsh accusations at a colleague.
It’d be great if we could identify the circumstances that lead up to emotional hijacks before they happen, but that’s not usually how it works. But learning to analyze an emotional hijack after it happens can be almost as valuable.
I like to call this process the “emotional postmortem.”
Just like a medical or project postmortem, the goal of an emotional postmortem is to determine the cause of “death,” or failure. When you identify the cause for a hijack, you can devise a plan to help you avoid repeat episodes in the future.
Link to the rest at Inc.
Public Domain Day 2022
From The Duke University School of Law:
In 2022, the public domain will welcome a lot of “firsts”: the first Winnie-the-Pooh book from A. A. Milne, the first published novels from Ernest Hemingway and William Faulkner, the first books of poems from Langston Hughes and Dorothy Parker. What’s more, for the first time ever, thanks to a 2018 law called the Music Modernization Act, a special category of works—sound recordings—will finally begin to join other works in the public domain. On January 1 2022, the gates will open for all of the recordings that have been waiting in the wings. Decades of recordings made from the advent of sound recording technology through the end of 1922—estimated at some 400,000 works—will be open for legal reuse.
. . . .
Why celebrate the public domain? When works go into the public domain, they can legally be shared, without permission or fee. That is something Winnie-the-Pooh would appreciate. Community theaters can screen the films. Youth orchestras can perform the music publicly, without paying licensing fees. Online repositories such as the Internet Archive, HathiTrust, and Google Books can make works fully available online. This helps enable access to cultural materials that might otherwise be lost to history. 1926 was a long time ago. The vast majority of works from 1926 are out of circulation. When they enter the public domain in 2022, anyone can rescue them from obscurity and make them available, where we can all discover, enjoy, and breathe new life into them.
The public domain is also a wellspring for creativity. The whole point of copyright is to promote creativity, and the public domain plays a central role in doing so. Copyright law gives authors important rights that encourage creativity and distribution—this is a very good thing. But it also ensures that those rights last for a “limited time,” so that when they expire, works go into the public domain, where future authors can legally build on the past—reimagining the books, making them into films, adapting the songs and movies. That’s a good thing too! As explained in a New York Times editorial:
When a work enters the public domain it means the public can afford to use it freely, to give it new currency . . . [public domain works] are an essential part of every artist’s sustenance, of every person’s sustenance.
Just as Shakespeare’s works have given us everything from 10 Things I Hate About You and Kiss Me Kate (from The Taming of the Shrew) to West Side Story (from Romeo and Juliet), who knows what the works entering the public domain in 2022 might inspire? As with Shakespeare, the ability to freely reimagine these works may spur a range of creativity, from the serious to the whimsical, and in doing so allow the original artists’ legacies to endure.
. . . .
Books
- A. A. Milne, Winnie-the-Pooh, decorations by E. H. Shepard
- Ernest Hemingway, The Sun Also Rises
- Dorothy Parker, Enough Rope (her first collection of poems)
- Langston Hughes, The Weary Blues
- T. E. Lawrence, The Seven Pillars of Wisdom (later adapted into the film Lawrence of Arabia)
- Felix Salten, Bambi, A Life in the Woods
- Kahlil Gibran, Sand and Foam
- Agatha Christie, The Murder of Roger Ackroyd
- Edna Ferber, Show Boat
- William Faulkner, Soldiers’ Pay (his first novel)
- Willa Cather, My Mortal Enemy
- D. H. Lawrence, The Plumed Serpent
- H. L. Mencken, Notes on Democracy
. . . .
Movies Entering the Public Domain
- For Heaven’s Sake (starring Harold Lloyd)
- Battling Butler (starring Buster Keaton)
- The Son of the Sheik (starring Rudolph Valentino)
- The Temptress (starring Greta Garbo)
- Moana (docufiction filmed in Samoa)
- Faust (German expressionist classic)
- So This Is Paris (based on the play Le Réveillon)
- Don Juan (first feature-length film to use the Vitaphone sound system)
- The Cohens and Kellys (prevailed in a famous copyright lawsuit)
- The Winning of Barbara Worth (a Western, known for its flood scene)
Musical Compositions
- Bye Bye Black Bird (Ray Henderson, Mort Dixon)
- Snag It (Joseph ‘King’ Oliver)
- Gentlemen Prefer Blondes (Irving Berlin)
- Black Bottom Stomp (Ferd ‘Jelly Roll’ Morton)
- Someone To Watch Over Me (George Gershwin, Ira Gershwin)
- Nessun Dorma from Turandot (Giacomo Puccini, Franco Alfano, Giusseppe Adami, Renato Simoni)
- Are You Lonesome To-Night (Roy Turk, Lou Handman)
- When the Red, Red Robin Comes Bob, Bob, Bobbin’ Along (Harry Woods)
- Ke Kali Nei Au (“Waiting For Thee”) (Charles E. King), in 1958 renamed Hawaiian Wedding Song with new lyrics (English) by Hoffman & Manning
- Cossack Love Song (Otto Harbach, Oscar Hammerstein II, George Gershwin, Herbert Stothart)
Link to the rest at The Duke University School of Law
Happy Public Domain Day!
From Cory Doctorow via Medium:
On January 1, 2019 something extraordinary happened. For the first time since 1998, the American public domain got bigger.
What happened in 1998? Congress — led by Rep Sonny Bono — extended the copyright on all works by 20 years. Works that had already been in the public domain went back into copyright. Works that were in copyright got an extra 20 years. The public domain…froze.
This was a wanton, destructive act. The vast majority of works that the Sonny Bono Act covered were out-of-print and orphaned, with no known owner. Putting them back into copyright for 20 years prevented their reproduction, guaranteeing that many would vanish from the historical record altogether.
As to the minuscule fraction of works covered by the Act that were still commercially viable: the creators of those works had accepted the copyright bargain of life plus 50 years. Giving them more copyright on works they’d already produced could not provide an incentive to make anything more. All it did was transfer value from the public domain into a vanishing number of largely ultra-wealthy corporate private hands.
As to living, working creators: those who’d made new works based on public domain materials that went back into copyright found themselves suddenly on the wrong side of copyright. Their creative labor was now illegal. Any working, living creator that contemplated making a new work based on material from the once-public-domain was now faced with tracking down an elusive (or possibly nonexistent) rightsholder, paying lawyers to negotiate a license, and subjecting their work to the editorial judgments of the heirs of long-dead creators.
The Sonny Bono Act is often called the Mickey Mouse Act, a recognition of the extraordinary blood and treasure that Disney spilled to attain retroactive copyright extension. This extension ensured that Steamboat Willie — and subsequent Mickey Mouse cartoons, followed by other Disney products — would remain Disney’s for another two decades.
Link to the rest at Cory Doctorow via Medium
PG would modify the factual description in the OP with a small change - The Sonny Bono Act was pushed through by California congresswoman Mary Bono (Sonny Bono’s widow and Congressional successor). Sonny served from 1995-98 and Mary, after winning a special election to become Sonny’s replacement, served from 1998-2013 after she failed to win another re-election.
Prior to getting into politics, Sonny was a musical performer, the less-talented half of Sonny & Cher.
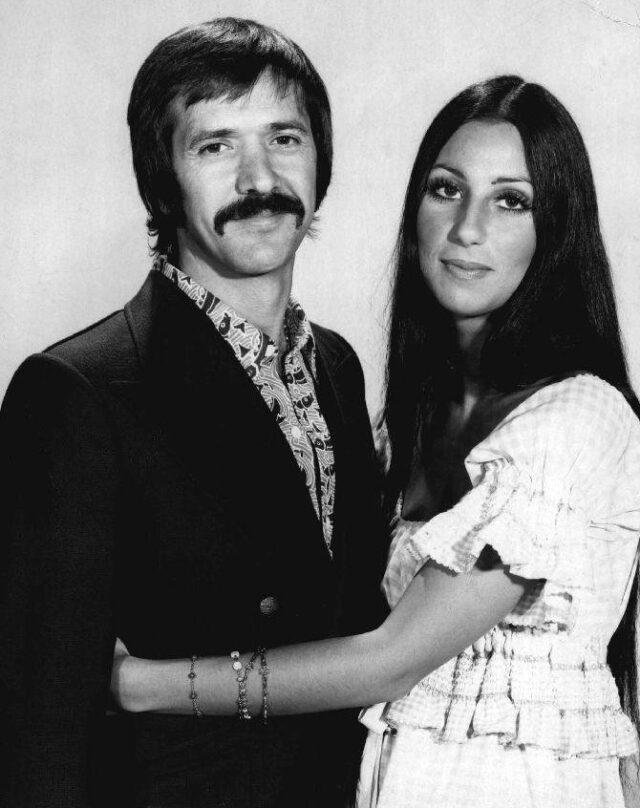
Sonny and Cher divorced in 1975 due to Sonny’s serial affairs with other women. Prior to marrying Sonny, his second wife, Mary, later Congresswoman Bono, had worked as a cocktail waitress and fitness instructor.
Sonny and Mary each represented the congressional district dominated by Palm Springs and nearby Palm Desert, retirement destinations for the wealthy and semi-wealthy which include a number of retired actors. Author Ann Rice (Interview with the Vampire, etc.) lived in Palm Springs until her death in 2021.
PG suggests the Bonos are yet another “only in California” stories.
Why good thoughts block better ones: the mechanism of the pernicious Einstellung effect
From The National Library of Medicine via PubMed:
Abstract: The Einstellung (set) effect occurs when the first idea that comes to mind, triggered by familiar features of a problem, prevents a better solution being found. It has been shown to affect both people facing novel problems and experts within their field of expertise. We show that it works by influencing mechanisms that determine what information is attended to. Having found one solution, expert chess players reported that they were looking for a better one. But their eye movements showed that they continued to look at features of the problem related to the solution they had already thought of. The mechanism which allows the first schema activated by familiar aspects of a problem to control the subsequent direction of attention may contribute to a wide range of biases both in everyday and expert thought - from confirmation bias in hypothesis testing to the tendency of scientists to ignore results that do not fit their favoured theories.
Link to the rest at PubMed
From Wikipedia:
Einstellung literally means “setting” or “installation” as well as a person’s “attitude” in German. Related to Einstellung is what is referred to as an Aufgabe (“task” in German). The Aufgabe is the situation which could potentially invoke the Einstellung effect. It is a task which creates a tendency to execute a previously applicable behavior. In the Luchins and Luchins experiment a water jar problem served as the Aufgabe, or task.
The Einstellung effect occurs when a person is presented with a problem or situation that is similar to problems they have worked through in the past. If the solution (or appropriate behavior) to the problem/situation has been the same in each past experience, the person will likely provide that same response, without giving the problem too much thought, even though a more appropriate response might be available. Essentially, the Einstellung effect is one of the human brain’s ways of finding an appropriate solution/behavior as efficiently as possible. The detail is that though finding the solution is efficient, the solution itself is not or might not be.
Another phenomenon similar to Einstellung is functional fixedness (Duncker 1945). Functional fixedness is an impaired ability to discover a new use for an object, owing to the subject’s previous use of the object in a functionally dissimilar context. It can also be deemed a cognitive bias that limits a person to using an object only in the way it is traditionally used. Duncker also pointed out that the phenomenon occurs not only with physical objects, but also with mental objects or concepts (a point which lends itself nicely to the phenomenon of Einstellung effect.
Link to the rest at Wikipedia
An 8-year-old slid his handwritten book onto a library shelf. It now has a years-long waitlist.
From The Washington Post:
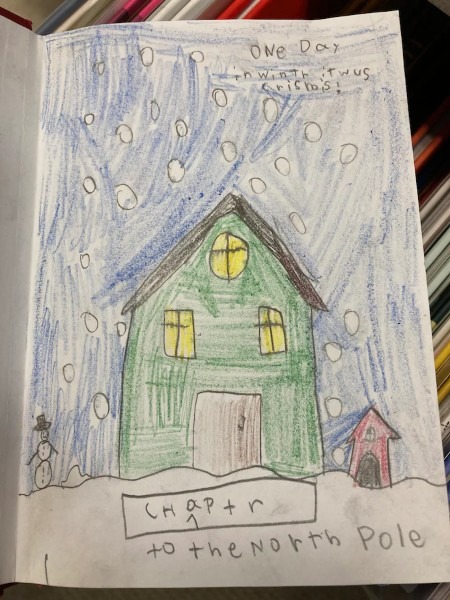
Dillon Helbig, a second-grader who lives in Idaho, wrote about a Christmas adventure on the pages of a red-cover notebook and illustrated it with colored pencils.
When he finished it in mid-December, he decided he wanted to share it with other people. So much, in fact, that he hatched a plan and waited for just the right moment to pull it off.
Days later, during a visit to the Ada Community Library’s Lake Hazel Branch in Boise with his grandmother, he held the 81-page book to his chest and passed by the librarians. Then, unbeknown to his grandmother, Dillon slipped the book onto a children’s picture-book shelf. Nobody saw him do it.
“It was naughty-ish,” Dillon, 8, said of covertly depositing the book without permission. But the result, he added, is “pretty cool.”
The book, titled “The Adventures of Dillon Helbig’s Crismis,” is signed “by Dillon His Self.”
He later confessed to his mother, Susan Helbig, that he slid his book into the stacks and left it there, undetected. But when they returned about two days later, to the spot where he left the notebook, it was missing. Helbig called the library to ask whether anyone had found Dillon’s notebook and to request that they please not throw it away.
Branch manager Alex Hartman said he was surprised at Dillon’s bold move.
“It was a sneaky act,” said Hartman, laughing. But Dillon’s book “was far too obviously special an item for us to consider getting rid of it.”
Hartman and a few co-workers had discovered and read Dillon’s book — which describes his adventures putting an exploding star on his Christmas tree and being catapulted back to the first Thanksgiving and the North Pole. They found it very entertaining.
Hartman read the book to his 6-year-old son, Cruzen, who giggled and said it was one of the funniest books he’d ever known.
“Dillon is a confident guy and a generous guy. He wanted to share the story,” Hartman said. “I don’t think it’s a self-promotion thing. He just genuinely wanted other people to be able to enjoy his story. … He’s been a lifelong library user, so he knows how books are shared.”
The staff librarians who read Dillon’s book agreed that as informal and unconventional as it was, the book met the selection criteria for the collection in that it was a high-quality story that was fun to read. So, Hartman asked Helbig for permission to tack a bar code onto the book and formally add it to the library’s collection.
Dillon’s parents enthusiastically said yes, and the book is now part of the graphic-novels section for kids, teens and adults. The library even gave Dillon its first Whoodini Award for Best Young Novelist, a category the library created for him, named after the library’s owl mascot.
. . . .
As luck would have it, the lone copy of “The Adventures of Dillon Helbig’s Crismis” has become a book in demand.
KTVB, a news station in Boise, reported on Dillon’s book caper earlier this month, and since then, area residents have begun adding themselves to a waiting list to check it out. As of Saturday, there was a 55-person waitlist.
. . . .
Dillon is also writing a different book about a closet that eats up jackets.
Link to the rest at The Washington Post
There is nothing like the death of a moneyed member of the family
There is nothing like the death of a moneyed member of the family to show persons as they really are, virtuous or conniving, generous or grasping. Many a family has been torn apart by a botched-up will. Each case is a drama in human relationships — and the lawyer, as counselor, draftsman, or advocate, is an important figure in the dramatis personae. This is one reason the estates practitioner enjoys his work, and why we enjoy ours.
Jesse Dukeminier and Stanley M. Johanson, estate planning attorneys
Books about Estate Planning and Authors
PG took a look on Amazon to locate books on the topic. He hasn’t reviewed any of these books and warns one and all that a book is not a substitute for a competent attorney familiar with estate planning and intellectual property issues.
One caveat - While the Federal Estate Tax is uniform across all states, each state has its own laws governing estates and trusts and its own laws regarding the probate of wills and state inheritance taxes. Some states don’t have state inheritance taxes.
This is why, you’ll want to look for an attorney who is experienced estate planning in your state. Should you move to a different state after creating a will and/or trust, you’ll want to have an experienced estate planning attorney practicing in your new state domicile review your current estate plan documents.
A Primer on Estate Planning as a Writer
From Jane Friedman:
Awareness of estate planning issues can be especially important to writers because of the unique nature of property rights in written works. Proper planning ensures that the ownership of a writer’s works after his or her death will end up in safe and knowledgeable hands.
In addition to giving the writer significant posthumous control over his or her works, an estate plan can greatly reduce the overall amount of estate tax paid at death. Because valuations of written works for estate tax purposes are not precise, estate taxes may turn out to be significantly higher than might have been anticipated. Thus, it is very important for writers to reduce their taxable estate as much as possible.
An estate plan may be either will-based or trust-based. Each type has advantages, but both are legitimate forms of estate planning. Estate laws and probate procedures vary throughout the United States, and a plan that works well for one person in one state may be inappropriate in other situations. Proper estate planning requires a knowledgeable lawyer and sometimes the assistance of other professionals, such as life insurance agents, accountants, and bank trust officers.
The Will
A will is a unique document in two respects. First, if properly drafted, it is ambulatory, meaning it can accommodate change, such as applying to property acquired after the will is made. Second, it is revocable, meaning it can be changed or canceled before death.
When carefully prepared, wills not only address how the assets of the estate will be distributed, but also foster better management of the assets. Those persons responsible for administering the estate of a decedent are known as executors in some states and personal representatives in others. It may be a good idea for writers to appoint joint executors so that one has publishing or writing experience and the other has financial expertise. In this way, the financial decisions can have the benefit of at least two perspectives. If joint executors are used, it will be necessary to make some provision in the will for resolving any deadlock between the two. A lawyer’s help will be necessary to set forth all of these important considerations in legally enforceable, unambiguous terms.
It is essential to avoid careless language that might be subject to attack by survivors unhappy with the will’s provisions. A lawyer’s help is also crucial to avoid making bequests that are not legally enforceable because they are contrary to public policy.
Trusts
A common way to transfer property outside the will is to place the property in a trust that is created prior to death. A trust is simply a legal arrangement by which one person holds certain property for the benefit of another. The person holding the property is the trustee; those who benefit are the beneficiaries.
To create a valid trust, the writer must identify the trust property, make a declaration of intent to create the trust, transfer property to the trust (this is often a step that is missed and can create a multitude of problems), and name identifiable beneficiaries. Failure to name a trustee will not defeat the trust, since if no trustee is named, a court will appoint one. (The writer may name himself or herself as trustee.)
Trusts can be created by will, in which case they are termed testamentary trusts, but these trust properties will be probated along with the rest of the will. To avoid probate, the writer must create a valid inter vivos or living trust.
Advantages of Using a Trust
The use of trusts to prepare a trust-based plan will, in certain situations, have significant advantages over a traditional will-based plan. For example, the careful drafting of trusts can allow the writer’s estate to avoid probate, which in some states is a lengthy and expensive process. Similarly, the execution of an estate through a trust-based plan can ensure a level of privacy not possible in probate court. Although these kinds of provisions provide some control over the estate, writers are cautioned that trusts cannot adequately substitute for a will if used haphazardly. Professional assistance is strongly recommended.
Link to the rest at Jane Friedman
PG says that dying without a will and/or trust usually ends up being the most expensive and time-consuming way of handling an estate for an author or anyone else.
That said, a poorly-drafted will can also cause an immense amount of difficulty and expense.
As mentioned previously, you’re looking for an estate planning attorney who can answer your questions, including questions about state and federal death taxes and how to minimize them.
Large law firms will have estate planning attorneys, but are likely to charge more for a similar service than a medium-sized or smaller law firm. That said, the amount of the fee a large firm charges for creating an estate plan will cost less than a legal dispute about your estate after you die.
As mentioned in comments to a prior post, you will want to make certain your estate-planning attorney is familiar with the special issues that can arise with intellectual property. If you have any concerns about an estate planning attorney’s appreciation of copyright issues, it will be worth it to ask her/him to associate counsel specializing in intellectual property, preferably copyright law (as opposed to patents, trademarks, trade secrets, etc.).
PG suggests accessing online information about authors and estate planning to become generally familiar with issues, jargon, etc. Check more than one or two sites so you’re not getting someone’s pet theories, peeves, etc.
For the record, although PG has done some estate planning for authors and others, he doesn’t do so any more.
Estate Planning for Authors
Since PG’s previous post about authors and their estates generated some good comments, he decided to post again on the topic.
The leading cause of death
The leading cause of death among fashion models is falling through street grates.
Dave Barry
When a Writer Dies: Making Difficult Decisions About the Work Left Behind
From Jane Friedman:
Nine days before my wife died, she forwarded me a Brevity post, The Death of a Writer, which asked:
Who is going to deal with your literary legacy, and what do you want done?
My wife wrote, “…interesting re what to do…”
She added a lifesaver emoji.
My wife, Mary Ann Hogan, journalist and teacher, died June 13, 2019, her “tango with lymphoma” ended, her life’s literary work unfinished.
Her manuscript explored her relationship with her father, William Hogan, longtime literary editor of the San Francisco Chronicle. Though he spent his life writing about books, Bill Hogan never wrote one of his own.
Mary Ann died thinking her book would redeem them both.
. . . .
My wife’s friends and writing partners agreed to help me read and judge what to save for the book or elsewhere. Then there would be drafts of the book to react to and fact-check. Her posse was more than willing. Mine, too.
We puzzled over things such as:
Should the final chapter be in my voice or hers? Both, we said. I would not pretend to be her. But I would quote her all the time, and we found those quotes.
What about the references to mental illness? She talked about panic attacks and flying thoughts, but never named the various diagnoses. What about wine? She talked about how she and her father all were big drinkers, without details. Leave it as she wrote it, we said.
What about the title? Circle Way came from the posse. Larger illustrations? That idea came from her writing mentor.
Rewrites? Mary Ann had created a lyric essay that jumped around like Kurt Vonnegut’s Slaughterhouse-Five, becoming at times a duet with her late father’s journal entries. This mosaic, we said, is best as is.
There’s more of her work to publish, in time, and now that we have a system, it can happen.
Finishing Mary Ann’s manuscript was not as hard as finding the right publisher. Parts of Circle Way had won three writing competitions. Publishers said it was “beautiful.” They also said it was “too literary” for the commercial marketplace.
My promise to my wife—to finish her book—felt shattered.
Now what?
Link to the rest at Jane Friedman
PG won’t spend much time on this, but talk to an attorney and get a will and/or a trust in place before you die or become incapacitated. Dying without a will is the most time-consuming and expensive way of passing your assets on to your heirs.
Writing a will is anything but rocket science, but if you have significant assets (more than a few hundred thousand dollars) or unusual types of property (like books you have written and self-published or books you’ve had published by any sort of publisher because whoever inherits the rights to those books will be able to collect royalties on them for the next 70 years in the US and a similarly long time in other nations recognizing copyright), the amount of money you spend to talk to an attorney and get her/his assistance will be tiny compared to the legal expenses of cleaning up an estate that hasn’t been handled properly.
Amazon is closing Westland, the Indian publishing company it acquired in 2016. What will happen to its catalogue and authors?
From The New Publishing Standard:
Amazon’s latest triumph of hope over experience comes to an end with the slow realisation that the India publishing industry, even if you own the largest digital platform in the world and have bought a successful home-grown publishing house with some of the country’s biggest author brands, is not a get rich quick scheme.
India has long been a triumph of hope over experience for Amazon, which has invested billions in the hope of one day returning profit from this huge market of 1.4 billion people, 755 million of whom are online.
. . . .
We don’t know, and likely never will, whether Westland ran at a loss for Amazon, but we can safely say Amazon is taking a loss by not selling on the company, rather choosing to close it down and absorb the human assets into the system. That of course being a reflection of how Amazon does business, not of Westland. Amazon buys, grows and profits from its acquisitions or buries them, to ensure a competitor doesn’t pick up the pieces.
In this case Amazon acquired Westland from Tata Trent back in 2016, and of course used its own platform to promote the books of its publishing company, just as it does APub – although interestingly Amazon never sought to meld Westland with APub.
New Tools: Indie Publishing
From Kristine Kathryn Rusch:
A theme of this year in review has been the hard split between indie publishing and traditional publishing. That split became clear in the numbers in 2021. The industry is no longer one industry. It’s at least two, maybe more.
But for now, we’ll go with two—indie and traditional. And one thing that has always separated these two industries is their willingness to grow and change. Indies are willing to change; traditional publishers are not.
One reason is that indie writers, in particular, are nimble enough to try new things and not have those things wreck their businesses or their business plans. An indie writer can take a book and make it exclusive in a new service for six months, and learn something. A traditional publisher has to make a legal commitment and usually cannot leave whatever service they’ve joined for a particular amount of time.
That makes sampling new tech and new software very difficult.
Also, much of the new tech is designed for the nimble indie, not for the big bloated traditional publisher. Which is why the new tools section is part of the indie publishing section of my year in review.
Many of these new tools are useless to traditional publishers. Others are impossible to sample, because the licensing agreements (contracts) those publishers have with their authors did not envision the latest, newest grandest thing. (That “any new tech anywhere in the universe” clause usually doesn’t cut it.)
. . . .
Bookstores
Generally speaking, the bookstores that survived that initial pandemic shut down from March to mid-summer 2020 are leaner and a lot more tech savvy. These stores, for the most part, are run by younger people. The older bookstore owners retired in that tough period or sold their stores. A lot of stores closed, particularly used stores. (Which is the position that Las Vegas is in. We had three used bookstores before March of 2020, and none now.)
Again, generally speaking, the new younger booksellers are more open-minded, a lot more willing to use the internet for everything from ordering to shipping, and receptive to local authors, even those not traditionally published.
All the information I have on this is either anecdotal or from the mists of my summer business reading. The good news here, though, is that indies who have paper editions can probably get them into a local bookstore, if only for a short time, provided the books look good (so many indie-designed paper books do not, even with all the best tools in the world), and provided the indie is willing to work with the store.
. . . .
One other U.S. bookstore development features Barnes & Noble, a company that seems to me like a mash-up between the Black Knight from Monty Python and The Holy Grail (“I’m fine”) and another Holy Grail sequence (“Not Dead Yet”). Barnes & Noble’s CEO since 2019, James Daunt, used the 2020 bookstore closures to remodel and remake the stores.
Then he did something rather brilliant—he returned control of each store to the local managers. They are now stocking books that locals ask for and want, rather than relying on corporate for ordering. Relying on corporate for ordering allowed B&N in the bad old days to get deep discounts on books, but it also meant that each store looked the same no matter where you went. And if a local author’s books were not in the store, nothing anyone could do would get them there. A special order only brought in one copy.
That’s changed, for right now anyway. Anecdotal reports are that the bookstores look bright and clean and full. The content is different from store to store, which makes the stores interesting.
From a writer’s point of view, suddenly the local chain store might be willing to order copies of a good-selling ebook or of a local author’s work for their local author section (if they have one). Writers actually have a chance to get their books into a brick-and-mortar store, at least one near their home.
Does all of this mean that B&N will stick around? Hell if I know. I don’t know if their balance sheet is good or bad anymore or what the changes mean.
But for 2022, anyway, the outlook is bright for anyone who wants to get their books into a nearby B&N. For what it’s worth.
Ebookstores
There are so many now that I can’t keep track. Companies here, there, and everywhere. Any indie who is not using tools like Draft2Digital to upload their books to very small e-retailers is missing an important cash stream. It seems that every time I go on D2D or, more often, use its referral arm, Books2Read, I see yet another store I haven’t heard of.
So the continual growth of e-retailers is something that has gone on for years now. But the biggest change on this front isn’t the retail companies. It’s the success of retail stores on individual author sites.
This is anecdotal, of course, because there’s no way to aggregate it. But the pandemic changed buying habits, introducing a lot of reluctant people to buying from sites other than the big retailers like Amazon and Walmart. That change in buying habits means that a lot of readers want to buy directly from the author.
So individual online bookstores went from being a silly waste of time to something that provides writers with their purest income—no one takes a percentage from their online store. The writers can control pricing, sales, and everything else.
It helps that online stores are easy to build now. There are a lot of tools that reduce the build to an easy upload, and a click or two. These programs also provide a secure checkout as well.
If you haven’t tried any of the online store programs for the past five years or so, then you’ll be surprised at how easy it all is for writer and consumer alike. I personally think this will be one of the major growth areas of 2022.
If there are only one or two things you can add to your plate this year, make designing and maintaining an online ebook store one of them.
Book Design Tools
Every few years or so there is a major improvement in indie book design. The last one I was aware of was the arrival of Vellum, a software program for Macs only. At first, Vellum was only for ebooks, and then it expanded to paper books. The Mac users swore by it, and I know that WMG changed a lot of its templates so that we could use Vellum, saving hours and hours of work on each book.
But, as I said above, Vellum is Mac-only. PC users bitched about that. There was a workaround—they could use Mac on cloud, but it had problems that made the workaround uncomfortable at best.
Now there’s Atticus, which works on all platforms, or so it says. The PC people are excited about it for that reason. But I’m also hearing that it’s a good design program.
Honestly, it really doesn’t matter if it’s good or not. Because next year, there will be another program, and two years from now, another. We’ve moved out of the stage where everyone who is publishing indie is using the same tools for the same work. We’re not even doing the same work—which is probably a topic for a future blog post.
As I’ve mentioned in this series, the longer we indies exist, the more companies try to cater to us. Or rather, to all of us in the arts. For a long time, Adobe offered the best platform to help with design and producing ebooks.
Other products either didn’t have the reach or the level of protocols. That’s changing. Affinity has become very competitive, and I know of several designers who prefer their ecosystem. I’m sure we will end up with more such tools as the decade progresses.
Link to the rest at Kristine Kathryn Rusch
Here’s a link to Kris Rusch’s books. If you like the thoughts Kris shares, you can show your appreciation by checking out her books.
6 Cheats to “Tell” Well (When It’s Warranted)
From Writers Helping Writers:
Most of us are familiar with the “Show, don’t Tell” rule. In short, it’s more effective to dramatize the story than to simply tell what happened. Nonetheless, almost every story needs at least some telling. It can help keep the pacing tight, relay background information, and enhance tone, among other things. Here’s more on when breaking the rule can work. So how do we tell well? Here are six cheats to help you.
1. Appeal to the Senses
Good showing appeals to the senses. Basically, we have to appeal to the senses to really show a story. There is no reason moments of telling can’t appeal to the senses in a similar way. Appealing to sight, sound, smell, taste, or touch can strengthen your telling just as it does with showing. It’s just that with telling, it’s usually brief, or relayed “in passing.” This example appeals to senses despite it being a telling summary:
We drove through Georgia, Alabama, Tennessee, Kentucky, stopping to cool the engine in towns where people moved with arthritic slowness and spoke in thick strangled tongues . . . At night we slept in boggy rooms where headlight beams crawled up and down the walls and mosquitoes sang in our ears, incessant as the tires whining on the highway outside. – This Boy’s Life by Tobias Wolff
2. Use Concrete Metaphors and Similes
Some telling doesn’t lend itself to the senses very easily, because of the subject matter that needs to be told. In cases like that, you can try tying in a concrete comparison to suggest a sense. This example tells about a telepathic and emotional connection using comparisons:
At night awake in bed, he’d remember her presence. How their minds had been connected, ethereal like spider webs. How just her being there brought a sense of comfort, like a childhood blanket he hadn’t realized he’d still had.
3. Sprinkle in Details
Just as you use detail to make your showing great, you can and often should include detail in passages of telling. Mention a red leather jacket here or a specific cologne there. Of course, you won’t be including as much detail as you would with showing, but detail makes telling more realistic. One key to making this work is to pick the right details, as opposed to generic ones.
Their mom had always stressed the importance of eating dinner as a family, of stir fry nights and cloth napkins on laps, of hands held in prayer and laughter pealing off travertine, and even of the occasional green bean food fight.
Link to the rest at Writers Helping Writers
Who owns how much of Harry Potter?
From The New York Times (9 February 2008):
On Friday, a lawyer named Anthony Falzone filed his side’s first big brief in the case of Warner Bros. Entertainment and J.K. Rowling v. RDR Books. Falzone is employed by Stanford Law School, where he heads up the Fair Use Project, which was founded several years ago by Lawrence Lessig, perhaps the law school’s best-known professor. Falzone and the other lawyers at the Fair Use Project are taking the side of RDR Books, a small book publisher in Muskegon, Michigan, which is the defendant.
As you can see from the titans who have brought the suit, RDR Books needs all the legal firepower it can muster.
As you can also probably see, the case revolves around Harry Potter. Rowling, of course, is the creator of the Harry Potter series - “one of the most successful writers the world has ever known,” crowed Neil Blair of the Christopher Little Literary Agency, which represents her. Warner Brothers, meanwhile, holds the license to the Harry Potter movies. And though Warner appears to be footing much of the bill, Rowling appears to be the party driving the litigation.
“I feel as though my name and my works have been hijacked, against my wishes, for the personal gain and profit of others and diverted from the charities I intended to benefit,” she said in a declaration to the court.
And what perfidious act of “hijacking” has RDR Books committed? It planned to publish a book by Steven Vander Ark, a former school librarian who for the past half-decade or so has maintained a fan site called the Harry Potter Lexicon. The Lexicon prints Harry Potter essays, finds Harry Potter mistakes, explains Harry Potter terminology, devises Harry Potter timelines, and does a thousand other things aimed at people who can’t get enough Harry Potter. In sum, it’s a Harry Potter encyclopedia for obsessive fans.
So long as the Lexicon was a Web site, Rowling looked kindly upon it; she once gave it an award and claimed to use it herself at times. But when Vander Ark tried to publish part of the Lexicon in book form - and (shudder!) to make a profit from his labors - Rowling put her foot down. She claims that she hopes to publish her own encyclopedia someday and donate the proceeds to charity; a competing book by Vander Ark would hurt the prospects for her own work.
But more than that, she is essentially claiming that the decision to publish, or to license, a Harry Potter encyclopedia is hers alone, since, after all, the characters in her books came out of her head. They are her intellectual property. And in her view, no one else can use them without her permission.
“There have been a huge number of companion books that have been published,” Blair said. “Ninety-nine percent have come to speak to us. In every case they have made changes to ensure compliance. They fall in line.” But in the case of the Lexicon, he said, “these guys refused to contact us.”
“They refused to answer any questions,” Blair said. “They refused to show us any details.”
They fall in line. There, in that one angry sentence, lies the reason that Falzone and his colleagues have agreed to help represent RDR Books. And in a nutshell, it’s why Lessig decided to start the Fair Use Project.
It’s a tad ironic that this dispute centers on a book, because ever since the recording industry began suing Napster, most of the big legal battles over copyright have centered on the Internet. The lawsuit Viacom filed against YouTube last year to prevent people from posting snippets of Viacom’s copyrighted television shows is the most obvious recent example.
But if you look a little further back, you’ll see that for a very long time now, copyright holders have made a series of concerted efforts to both extend copyright protection, and to make it an ever-more powerful instrument of control. More than a century ago, copyrights lasted for 14 years - and could be extended another 14 if the copyright holder petitioned for the extension. Today, corporate copyrights last for 95 years, while authors retain copyright for 70 years after their death. The most recent extension of copyright, passed by Congress in 1998, was driven in no small part by Disney’s desire to prevent Mickey Mouse and several of its other classic cartoon characters from falling into the public domain.
. . . .
At the same time, though, copyright holders have tried to impose rules on the rest of us - through threats and litigation - that were never intended to be part of copyright law. They sue to prevent rappers from taking samples of copyrighted songs to create their own music. Authors’ estates try to deprive scholars of their ability to reprint parts of books or articles because they disapprove of the scholar’s point of view. Lessig likes to cite a recent, absurd case where a mother put up on YouTube a video of her baby dancing to the Prince song “Let’s Go Crazy” - and Universal Music promptly sent her a cease-and-desist letter demanding that she remove the video because it violated the copyright.
There is no question that these efforts have had, as we like to say in the news business, a “chilling effect.” Roger Rapoport, who owns RDR Books, told me that ever since the case was filed, he has heard dozens of horror stories. “One university publisher told me they have given up literary criticism because of this problem,” he said.
. . . .
About a decade ago, though, Lessig decided to fight back. His core belief is that copyright protection, as he put to me, “was meant to foster creativity, not to stifle it” - yet that is how it is now being used. He fought the copyright extension of 1998 all the way to the Supreme Court. (He lost.) He founded a group called Creative Commons, which is, in a sense, an alternative form of copyright, allowing creators to grant far more rights to others than the traditional copyright system. And he founded the Fair Use Project to push back against, well, against copyright hogs like Rowling.
No one is saying that anyone can simply steal the work of others. But the law absolutely allows anyone to create something new based on someone else’s art. This is something the Internet has made dramatically easier - which is part of the reason why we’re all so much more aware of copyright than we used to be. But it has long been true for writers, film-makers and other artists. That’s what “fair use” means.
And that is what is being forgotten as copyright holders try to tighten their grip. Documentary film makers feel this particularly acutely, for instance. My friend Alex Gibney, who directed the recent film “Taxi To The Dark Side,” about torture, tried to get Fox to license him a short clip from the television series “24” to illustrate a point one of his talking heads was making about how the show portrays the use of torture at the CIA. Fox denied his request. Gibney, a fair use absolutist, used it anyway - but many filmmakers would have backed away.
Which is also why the Harry Potter Lexicon case is so important. For decades, fair use has been thought to extend to the publication of companion books that build on the work of someone else - so long as the new work adds something new and isn’t simply a rehash of the original. There are dozens of companion books to the Narnia chronicles, for instance, or the works of J.R.R. Tolkien.
. . . .
And, in a roundabout way, that gets us back what the Internet has wrought. For, as Lessig points out, “anybody who owns a $1,500 computer” can now create culture that is based on someone else’s creation. Indeed, we do all the time - on Facebook, on YouTube, everywhere on the Internet. If the creation of that content is deemed to be a violation of copyright, Lessig said, “then we have a whole generation of criminals” - which is terribly corrosive to the society. But if it is fair use, as it ought to be, then it becomes something quite healthy - new forms of free expression and creativity.
Link to the rest at The New York Times
From the U.S. Copyright Office:
More Information on Fair Use
Fair use is a legal doctrine that promotes freedom of expression by permitting the unlicensed use of copyright-protected works in certain circumstances. Section 107 of the Copyright Act provides the statutory framework for determining whether something is a fair use and identifies certain types of uses—such as criticism, comment, news reporting, teaching, scholarship, and research—as examples of activities that may qualify as fair use. Section 107 calls for consideration of the following four factors in evaluating a question of fair use:
- Purpose and character of the use, including whether the use is of a commercial nature or is for nonprofit educational purposes: Courts look at how the party claiming fair use is using the copyrighted work, and are more likely to find that nonprofit educational and noncommercial uses are fair. This does not mean, however, that all nonprofit education and noncommercial uses are fair and all commercial uses are not fair; instead, courts will balance the purpose and character of the use against the other factors below. Additionally, “transformative” uses are more likely to be considered fair. Transformative uses are those that add something new, with a further purpose or different character, and do not substitute for the original use of the work.
- Nature of the copyrighted work: This factor analyzes the degree to which the work that was used relates to copyright’s purpose of encouraging creative expression. Thus, using a more creative or imaginative work (such as a novel, movie, or song) is less likely to support a claim of a fair use than using a factual work (such as a technical article or news item). In addition, use of an unpublished work is less likely to be considered fair.
- Amount and substantiality of the portion used in relation to the copyrighted work as a whole: Under this factor, courts look at both the quantity and quality of the copyrighted material that was used. If the use includes a large portion of the copyrighted work, fair use is less likely to be found; if the use employs only a small amount of copyrighted material, fair use is more likely. That said, some courts have found use of an entire work to be fair under certain circumstances. And in other contexts, using even a small amount of a copyrighted work was determined not to be fair because the selection was an important part—or the “heart”—of the work.
- Effect of the use upon the potential market for or value of the copyrighted work: Here, courts review whether, and to what extent, the unlicensed use harms the existing or future market for the copyright owner’s original work. In assessing this factor, courts consider whether the use is hurting the current market for the original work (for example, by displacing sales of the original) and/or whether the use could cause substantial harm if it were to become widespread.
In addition to the above, other factors may also be considered by a court in weighing a fair use question, depending upon the factual circumstances. Courts evaluate fair use claims on a case-by-case basis, and the outcome of any given case depends on a fact-specific inquiry. This means that there is no formula to ensure that a predetermined percentage or amount of a work—or specific number of words, lines, pages, copies—may be used without permission.
Please note that the Copyright Office is unable to provide specific legal advice to individual members of the public about questions of fair use.
Link to the rest at U.S. Copyright Office
PG says that, while there are areas of legal clarity regarding what is and what is not fair use under US copyright law, the boundary between those two sets of rights includes some gray areas.
If you look at the Copyright Office explanation above, you’ll find a list of fundamental descriptions of fair use:
- Purpose and character of the use, including whether the use is of a commercial nature or is for nonprofit educational purposes
- Nature of the copyrighted work
- Amount and substantiality of the portion used in relation to the copyrighted work as a whole
- Effect of the use upon the potential market for or value of the copyrighted work
Concepts like purpose and character of the use, amount and substantiality of the portion used and effect of the use upon the potential market include a number of bright legal lines, but have also left quite a lot of gray areas that have been the subject of lots of litigation.
In the nature of litigation decisions, the more valuable the copyright, the more likely the owner of the copyright (or her attorneys) will be to carefully examine each instance where a work by another author seems similar in some ways to the original creation.
In addition to infringing the creator’s copyright, there is also an issue of trademark rights. As a general proposition, the title of a book is not protectable as a trademark. That said, “Harry Potter” is definitely a trademark and if you decide to publish a book titled, “Harry Potter and The Grinch,” you’re likely to hear from Ms. Rowling (or maybe Warner Brothers) and attorneys for Dr. Seuss Enterprises, L.P.
Here’s a link to the details about the U.S. trademark for The Grinch.
Pottermore heralds ‘exceptional’ year as profits soar by 150%
From The Bookseller:
Pottermore Publishing, the digital content company for J K Rowling’s Wizarding World, saw revenues rise by around a quarter to £40.4m while pretax profits rocketed 150% to £9.5m.
The company reported details of its financial results on 31st January covering the period for the 12 months to 31st March 2021. It has not yet made its accounts public at Companies House.
Revenues saw an uplift of 23% from £32.5m in 2020 to £40.4m while pretax profits soared from £3.8m to £9.5m.
The company said: “Pottermore Ltd had an exceptional year benefitting from a significantly increased appetite for digital reading during the pandemic, strong sales performance of the Harry Potter e-books and digital audiobooks and continued investment in franchise planning in partnership with Warner Bros.
“The Harry Potter At Home campaign, delivered by Wizarding World Digital LLC, further supported reading during the lockdown of 2020. This saw celebrities from the Wizarding World and beyond read from Harry Potter and the Philosopher’s Stone (Bloomsbury Children’s). The chapter reads were made available free of charge on www.wizardingworld.com. Pottermore Publishing also worked with partners such as Audible and Overdrive during this time to allow free access to the audio book and e-book of Harry Potter and the Philosopher’s Stone in multiple languages.”
Link to the rest at The Bookseller
‘Maus’ Tops Amazon Bestseller List After Tennessee School Board Pulls Graphic Novel
From The Wall Street Journal:
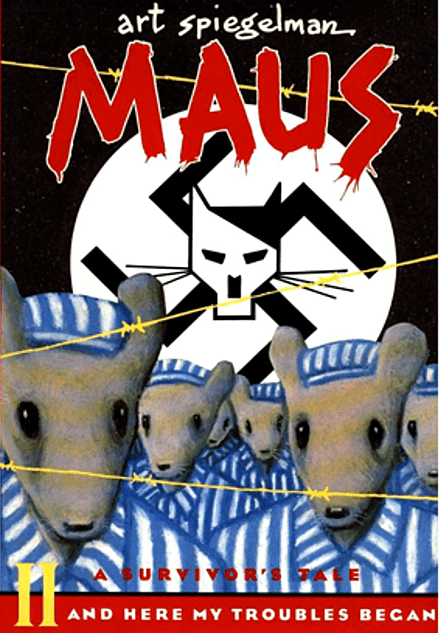
“Maus,” a graphic novel about the Holocaust published decades ago, reached the top of Amazon.com Inc.’s bestsellers list after a Tennessee school board’s decision to remove the book spurred criticism nationwide.
“The Complete Maus,” which includes the first and second installments of Art Spiegelman’s Pulitzer-Prize winning graphic novel, sat at the top of Amazon’s bestseller list Monday morning. It later moved to the No. 2 spot. Separate copies of the installments, published in 1986 and 1991, respectively, were also among the top 10 bestselling books on the retail giant’s website.
Attention to the graphic novel was renewed this month when the McMinn County Board of Education in Athens, Tenn., voted unanimously to remove “Maus” from its eighth-grade curriculum. The 10-member board cited “vulgar” words that appeared in the book as well as subjects they deemed inappropriate for eighth-graders.
The school board’s Jan. 10 decision sparked widespread criticism. In an interview with CNBC last week, Mr. Spiegelman said he was baffled by the move, calling it “Orwellian.” A representative for Mr. Spiegelman said he wasn’t available for further comment Monday.
. . . .
In “Maus,” Mr. Spiegelman examines the horrors of the Holocaust and his parents’ journey of survival, depicting Nazis as cats and Jewish people as mice. The nearly 300-page graphic novel received a special Pulitzer Prize in 1992.
The McMinn County Board of Education said the graphic novel “was simply too adult-oriented” and cited the use of profanity, nudity, and depictions of violence and suicide. In a statement last week, the board said it doesn’t dispute the importance of teaching students about the Holocaust and said it asked administrators to find more age-appropriate texts to “accomplish the same educational goal.”
“The atrocities of the Holocaust were shameful beyond description, and we all have an obligation to ensure that younger generations learn from its horrors to ensure that such an event is never repeated,” the board said in a statement last week. “We simply do not believe that this work is an appropriate text for our students to study.”
Link to the rest at The Wall Street Journal (PG apologizes for the paywall, but hasn’t figured out a way around it.)
Students Called Radicals by Superintendent Fundraise for Freedom to Read
From Book Riot:
On January 25th, Granbury Independent School District in Texas pulled 100 books for review based on Matt Krause’s list of 850 books he wants banned from school libraries. Five books were pulled from shelves. Students spoke out at the board meeting,
On January 25th, Granbury Independent School District in Texas pulled 100 books for review based on Matt Krause’s list of 850 books he wants banned from school libraries. Five books were pulled from shelves. Students spoke out at the board meeting, saying,
We want to learn about things that may not be the prettiest or the most comfortable, but we as students are entitled to complete knowledge…
In response, superintendent of the district Jeremy Glenn said,
We want to learn about things that may not be the prettiest or the most comfortable, but we as students are entitled to complete knowledge…
In response, superintendent of the district Jeremy Glenn said,
Let’s not misrepresent things. We’re not taking Shakespeare, Hemingway off the shelves, and we’re not going and grabbing every socially, culturally, or religiously diverse book and pulling them. That’s absurd. And the people that are saying that are gaslighters, and it’s designed to incite division.
He went on to discuss “radicals” in school board meetings that he claims are sowing division in the community.
The students speaking out at the school board meeting decided to take these accusations and use them to raise money to fight censorship.
. . . .
They are selling a tee shirt with the text “radical gaslighter” on it, and all proceeds go to the Freedom to Read Foundation.
Link to the rest at Book Riot
PG notes that this particular censorship apparently originated with right-wing critics. In the US in recent years, censorship and book bans have primarily been from the Woke left.
The cover version is a misunderstood musical form
From The Economist:
Chan marshall (pictured), who goes by the stage name Cat Power, has been a fixture on the American indie-rock scene since the mid-1990s. She is a highly regarded artist, praised for her sombre, powerful songwriting and sound. Her 11th album, “Covers”, a set of versions of previously recorded songs, was released this month. It will be the third such LP she’s put out, following “The Covers Record” (2000) and “Jukebox” (2008); they make up more than a quarter of her total album releases.
It is noteworthy that Ms Marshall, or any musician, makes the distinction between “covers” and “original music” at all. For the first six decades of the recorded-music era, which began in earnest in the early 20th century, there was a clear division of labour: writers wrote and singers sang. Two industries—the recording one, and the songwriting one—grew up in parallel. In America, the writing arm was nicknamed Tin Pan Alley, and the business was concentrated on a single Manhattan street. Tin Pan Alley’s early fortune lay in sheet music, and a popular song could sell in the millions.
As recorded music took over, professional songwriters remained in demand. Even the rock’n’roll era merely shifted the action 20 blocks north, to the Brill Building. Competing versions of numbers jockeyed for position in the charts; the idea that a song could belong to a particular artist, other than in a strict licensing sense, had little traction. A “standard” was just that—a song so widely performed that only a very special reading could affix it to any one artist.
Woody Guthrie and Hank Williams were prominent singer-songwriters in the early-to-mid-20th century, but both were anomalies. Two acts were chiefly responsible for a major shift in the early 1960s: Bob Dylan and The Beatles. These performers created a wider perception that the writer and the artist not only could be, but should be, one and the same. Their youthful stardom, aided by a new mass media (and television in particular), popularised the idea of the musical auteur. By 1985 Mr Dylan was in a position to boast that: “Tin Pan Alley is gone. I put an end to it. People can record their own songs now.”
This was an oversimplification. Work by Mr Dylan and the Beatles was at the time covered widely, and lucratively—in Mr Dylan’s case, often before he had released a recorded version, making him a kind of one-man Tin Pan Alley in himself. In the 2010s he recorded three consecutive sets of pre-rock’n’roll American pop standards, a loving tribute to the very songs he once claimed to have made obsolete.
This in turn raises the question: what exactly constitutes an “original”? Does a musician “cover” a songwriter, or a recording? Ms Marshall’s album features a version of “These Days”, written by Jackson Browne, and first recorded by Nico in 1967. Mr Browne would not release a version until 1973, and his iteration bore a notable resemblance to a country-rock arrangement issued by Greg Allman earlier that year. Ms Marshall’s spare, folky take steers closest to the Nico version (on which Mr Browne played a distinctive guitar part), and includes a verse Nico performed but Mr Browne later omitted. So is she covering Nico, or Mr Browne? To whom does the song “belong”?
You might argue that if it belongs to anybody, a song belongs to whoever delivers it most memorably. Elvis Presley was above all an interpreter, and a superb one. “Hound Dog”, “Blue Suede Shoes”, “Suspicious Minds” and (until Pet Shop Boys audaciously reworked it) “Always On My Mind” have long been thought of as “Elvis songs”, yet all are cover versions. Nina Simone and Johnny Cash—no mean songwriter, either of them—likewise possessed a gift for claiming spiritual ownership of any song they covered.
An outstanding cover version can wrest a song from the grasp of even the biggest stars. So commanding is Sinéad O’Connor’s “Nothing Compares To U”, for example, that it relegates the song’s author, Prince, to a footnote. Even Mr Dylan is not impervious to this phenomenon; when touring for the first time since he recorded it, he played his song “All Along The Watchtower” not in the subdued folk-pop style of the original of 1967, but as a searing blast of rock plainly indebted to the authoritative version of 1968 by the Jimi Hendrix Experience (pictured above). In effect, he was covering a cover of his own song.
Link to the rest at The Economist
PG says copyright is a wondrous and multi-faceted bundle of rights.
The difference between
The difference between false memories and true ones is the same as for jewels: It is always the false ones that look the most real, the most brilliant.
Salvador Dali
Losing native languages is painful. But they can be recovered
From The Economist:
Memory is unfaithful. As William James, a pioneering psychologist of the 19th and early 20th centuries, observed: “There is no such thing as mental retention, the persistence of an idea from month to month or year to year in some mental pigeonhole from which it can be drawn when wanted. What persists is a tendency to connection.”
Julie Sedivy quotes James in a poignant context in her new book “Memory Speaks”. She was whisked from Czechoslovakia with her family at the age of two, settling eventually in Montreal. In her new home she became proficient in French and English, and later became a scholar in the psychology of language. But she nearly lost her first language, Czech, before returning to it in adulthood. Her book is at once an eloquent memoir, a wide-ranging commentary on cultural diversity and an expert distillation of the research on language learning, loss and recovery.
Her story is sadly typical. Youngsters use the child’s plastic brain to learn the language of an adoptive country with what often seems astonishing speed. Before long it seems to promise acceptance and opportunity, while their parents’ language becomes irrelevant or embarrassing, something used only by old people from a faraway place. The parents’ questions in their home language are answered impatiently in the new one, the children coming to regard their elders as out-of-touch simpletons who struggle to complete basic tasks.
For their part, meanwhile, the parents cannot lead the subtle, difficult conversations that guide their offspring as they grow. As the children’s heritage language atrophies, the two generations find it harder and harder to talk about anything at all.
Children often yearn desperately to fit in. Often this can mean not only learning the new language, but avoiding putting off potential friends with the old. Children, alas, can also be little bigots. At the age of five, researchers have found, they already express a preference for hypothetical playmates of the same race as them. They also prefer friends who speak only their language over those who speak a second one as well.
In theory, keeping a language robust once uprooted from its native environment is possible. But that requires the continuance of a rich and varied input throughout a child’s development—not just from parents, but through activities, experiences, books and media. These are often not available in countries of arrival. Parents are themselves pressed to speak in the new language to their children, despite evidence that their ungrammatical and halting efforts are not much help.
But a dimming language may not be as profoundly lost as speakers fear when, as adults, they visit elderly relatives or their home countries and can barely produce a sentence. Though the language may not be as retrievable as it once was, with time and exposure it can be relearned far faster than if starting from scratch.
Link to the rest at The Economist
Making Numbers Count
From The Wall Street Journal:
When Alfred Taubman was chief executive of the restaurant chain A&W, he came up with a clever way of challenging the competition: He offered a third-pound burger for the cost of a McDonald’s quarter-pounder. The result? More than half of A&W’s customers seethed, convinced that they were being asked to pay the same amount for what sounded to them like a smaller burger.
One lesson from this episode: “Math is no one’s native tongue.” So observe Chip Heath and Karla Starr in “Making Numbers Count,” a close look at the challenge of understanding—and communicating—numerical claims. The authors note that, once we get beyond 1, 2, 3, our ability to grasp numbers quickly deteriorates; it’s better, if possible, to translate them into “concrete, vivid, meaningful messages that are clear enough to make numbers unnecessary.”
Consider how we might describe the world’s water: 97.5% is salinated; the other 2.5% is fresh water, but 99% of that amount is trapped in glaciers, leaving only a small fraction that is actually drinkable. If you want people to “see and feel the numbers, not just read them,” Mr. Heath and Ms. Starr say, consider a visual analogy: Imagine “a gallon jug filled with water with three ice cubes next to it.” The jug represents the earth’s salt water, the ice cubes the glaciers, and “the drops melting off each”—that’s what’s available for consumption. Another eye-catching comparison, this one taken from a 2018 New York Times article: Among Fortune 500 CEOs, there are more men named “James” than there are women in total.
One way to make numbers come alive is through stories, which our brains process “better than statistics.” We’re unlikely to remember details about desperately low wages and unconscionably high interest rates in Bangladesh, for example, but we can’t forget the story of the economist Muhammad Yunus’s efforts to distribute small, transformative loans to grateful recipients.
Often the use of numbers is unavoidable, as Mr. Heath, a business professor at Stanford, and Ms. Starr, a science writer, readily concede. What to do? Since we process “user-friendly numbers” much better than decimals and percentages (as A&W discovered to its dismay), simple analogies can be useful. Global health data, for instance, might be translated into a representative village of 100, in which 29 people would be overweight and 10 would be going hungry. We can also employ culturally relevant frames of reference. The 6-foot social-distancing guidance for Covid has been compared to a hockey stick (in Canada), a tatami mat (Japan), a surf board (San Diego) and an ostrich-like cassowary (Australia). Other comparisons—24 buffalo wings (Buffalo, N.Y.) and 72 (presumably giant) pistachios (New Mexico)—seem more clever than useful.
Link to the rest at The Wall Street Journal (PG apologizes for the paywall, but hasn’t figured out a way around it.)
A+ Content on Kindle Direct Publishing
From Kindle Direct Publishing:
PG stumbled on something he hadn’t seen before on KDP, A+Content capabilities.
Basically, this appears to be a new tool to allow you to perk up your indie book descriptions with breakthrough formatting such as Bold, images, images with text overlays and stuff your fourth-grade relative has been doing in html since three months after she/he was born.
However, instead of using sophisticated html creation programs, you have to use a clunky-looking set of tools that the bosses at KDP have ordered their underlings to create.
In addition, the Zon has special content guidelines that appear to be different than the usual KDP book description content guidelines.
To wit:
Before you create A+ Content, review the A+ Content Guidelines. Amazon has specific terms and policies regarding types of content that may not be allowed, so review these carefully. Violating these guidelines may lead to a rejection by our system, which can require updates.
Just because KDP has a marketplace where you’re promoting your books now doesn’t mean that it will support A+ Content.
A+ Content must be created and published in each marketplace where you would like it displayed. From kdp.amazon.com, you can publish A+ Content in these marketplaces:
- Amazon.com
- Amazon.ca
- Amazon.com.mx
- Amazon.com.br
- Amazon.co.uk
- Amazon.de
- Amazon.fr
- Amazon.es
- Amazon.in
- Amazon.it
- Amazon.nl
- Amazon.com.au
- From kdp.amazon.co.jp you can publish A+ Content in Amazon.co.jp
The languages that A+ Content can be published in vary by marketplace.
And, finally, the book description police have upped their game as well.
All content in compliance with our A+ Content Guidelines will appear on your detail page within eight business days. If your content requires changes, we’ll send you an email with further instructions.
For PG, this feels like going back to Web Design 1.0 again. You can check out Content Examples of A+ Content to see what the A+ people think is cool online merchandising.
Link to the rest at Kindle Direct Publishing
PG has speculated before that Amazon’s KDP tech and management people live in a world of their own that is apart from the mothership tech and design group. For Amazon’s other product lines, there are lots and lots of ways of presenting information, formatting marketing messages, putting up images, etc., etc.
You can even create your own branded store - here’s a link to one for Cuero, a leather-goods company PG hadn’t heard of before stumbling on it when he was looking for an example of a visually-interesting store on Zon.
For some reason books and authors seem to get the brown shoe set of marketing design tools. For example, if you look at JK Rowling’s author page, you’ll see that it looks pretty much like Rosie Graveltruck’s author page. Aside from her family, Rosie has not made any sales on Amazon. JK has been a money machine for both her publisher and the Zon. Cuero is way cooler than JK is.
PG just used a free app he found online while creating this post - PIXLR - to create an Author Page graphic that is far more eye-catching than Amazon can manage for JK.

When Is It Okay to Let a Bookstore Die?
From Book Riot:
Readers love bookstores. Even the most devoted library power user, audiobook aficionado, or ebook devotee enjoys wiling time away in the aisles. There’s perhaps nothing more romanticized in the bookish world than a secondhand bookstore brimming with stacks of books precariously balanced on every surface. They make for great Instagram pictures — but do they make for a good business model?
Speaking of romanticization, books are often conferred a certain status that almost no other object is. Reading isn’t just a hobby; it’s a lofty pursuit. Books aren’t just widgets; they’re sacred objects. Reading and books aren’t just associated with status and education. They’re also often associated with a kind of moral weight. It’s not unusual for everyone from BookTokers to booksellers to say they promote literacy, which certainly sounds like a noble pursuit.
Getting people to read (or buy) more books isn’t the same thing as promoting literacy, though, if we’re being completely honest. Increasing literacy would involve teaching people (whether kids or adults) the skills of reading, from the most basic phonics and decoding knowledge to more intricate strategies, like spotting motifs and themes, critically engaging with a text, and recognizing bias.
Convincing someone to pick up a random book doesn’t necessarily achieve any of those goals, and yet it still feels like a victory. Bookstores have an air of improving society, of being ethically superior to other businesses. When that veneer is scratched away, though, you’re left with a business that needs to make money. Apart from a handful of not-for-profit or communist/anarchist bookstores, they function in much the same way any other business does.
But while it’s fairly common for independent bookstores to do GoFundMe-style crowdfunding campaigns or to simply ask customers to place orders to keep the lights on, it’s unlikely that a local soap and cosmetics store or a boutique fashion location doing something like this would be received similarly. After all, they’re businesses. If they’re not profitable, why should they stay open?
. . . .
When I started working for a used bookstore, there were piles of books on the ground, and nothing was catalogued online. It was exactly the kind of ~aesthetic~ used bookstore you might see on Instagram. People would come in and exclaim at how lovely it was…and often those same people would leave after 15 minutes of looking around without buying anything. Because the stacks were overwhelming, they trapped dust, and they blocked shelves.
. . . .
Since then, the store has expanded (hooray!) and changed locations. There are no more piles on the floor, and everything is catalogued online. The booksellers there still have people come in and say how they miss the charm of the old store, and specifically that they miss the piles of books on the floor. The staff who had to spend hours moving piles of books around, lugging tubs of books up stairs without an elevator, and searching through the 18 places a title might be shelved largely disagree.
There’s a vision of used bookstores as tiny, cramped spaces filled from floor to ceiling with books in very little order at all. Tucked away in a corner is someone reading, who is likely cranky and will criticize your reading taste. They do not have the newest releases. The idea of finding a treasure in those piles is enticing, but it’s just not a sound business strategy most of the time, and it’s no surprise that these shops have largely disappeared. And that’s okay.
. . . .
Bookstores are not inherently morally superior to any other business, though, and sometimes they just aren’t a good fit. Maybe it isn’t run effectively. Maybe there aren’t enough customers or the rent is too high. Maybe the staff is condescending or unhelpful. Maybe there’s too much competition. I don’t think readers have an obligation to support every physical bookstore. Sometimes, it’s their time to shut up shop.
Link to the rest at Book Riot
PG isn’t certain exactly what the author of the OP is trying to demonstrate other than bookstores have a past.
PG agrees that “bookstores are not inherently morally superior to any other business” even though he enjoyed physical bookstores in the past.
The problem with physical bookstores today is entirely financial. After the rise of Barnes & Noble and Borders, only a relatively small group of people made much money owning/operating an independent bookstore. Long before Amazon showed up, a typical independent bookstore could expect an annual profit margin of 1-2%.
The widespread shutdown in the United States during the Age of Covid was disastrous for physical bookstores.
From the Open Education Database (PG thinks in 2002):
- Today, there are around 10,800 bookstores in the U.S.Though it might seem that bookstores are closing at a rapid pace, there are actually still an impressive amount of bookstores in the U.S.; about 10,800 in all, ranging from small, independent retailers to major chains, according to census data from 2002. Yet that number is considerably lower than the number recorded in 1997 when there were 12,363 stores, a 12.2% drop.
- There are more bookstores today than there were in 1930.
. . . .
- E-books have captured $3.2 billion of the market.E-books offer readers convenience and the chance to save money on buying books, but they’re also causing bookstores to take a major hit. In 2011, e-books captured $3.2 billion of the bookselling market, and by 2016 that number is projected to grow to nearly $10 billion. That estimate could be pretty close to reality based on past trends; between 2010 and 2011 alone e-book sales rose by 210% and comprised 30% of all sales of adult fiction. Prior to the introduction of the Amazon Kindle, the e-book market was fairly insignificant. Now, with nearly 28% of Americans owning an e-reader device, it’s not uncommon to see sales jump exponentially from year to year.
Link to the rest at Open Education Database
PG notes that the stats listed above are twenty years old.
From The United States Census:
According to data from the Census Bureau’s County Business Patterns . . . the number of U.S. Book stores . . . dropped from 12,151 in 1998 to 6,045 in 2019.
Link to the rest at The United States Census
PG suggests that sales from physical bookstores were under siege a long time before Amazon was founded in 1994. You’ll recall that Barnes & Noble and Borders put a large number of independent bookstores out of business during their rise to the top of the traditional bookstore market.
From The New York Times (October 15,2020):
The signs started appearing in bookstore windows this week.
“Buy books from people who want to sell books, not colonize the moon.”
“Amazon, please leave the dystopia to Orwell.”
“If you want Amazon to be the world’s only retailer, keep shopping there.”
The message: Buy from these shops, or they won’t be around much longer. According to the American Booksellers Association, which developed the campaign, more than one independent bookstore has closed each week since the pandemic began. Many of those still standing are staring down the crucial holiday season and seeing a toxic mix of higher expenses, lower sales and enormous uncertainty.
Even though book sales have been a bright spot in an exceedingly grim national economy — they rose more than 6 percent so far this year compared with last year, according to NPD BookScan — most of those purchases are not going through independent stores.
. . . .
Still, local independent stores have hustled and reinvented themselves during the pandemic. Mailing books to customers, which used to be a minuscule revenue stream for most shops, can now be more than half of a store’s income, or virtually all of it for places that are not yet open for in-person shopping. Curbside pickup has become commonplace.
Avid Bookshop in Athens, Ga., sends personalized URLs to customers with a list of handpicked recommendations. Green Apple Books in San Francisco raised $20,000 selling T-shirts, hoodies and masks that said “Stay home, read books.” Other stores have pleaded for customers to donate money.
All that still may not be enough.
“Somebody said to me, ‘Boy, you must be raking it in with all the online business you’re getting,’” said Christine Onorati, an owner of Word bookstores in Brooklyn and Jersey City, N.J. “It makes me laugh.”
Bookstores across the country face different challenges depending on any number of factors, including their local economies and how they have been affected by the coronavirus. But some broad trend lines have started to emerge, perhaps most of all that bigger, right now, is not better.
Take Vroman’s Bookstore, a 126-year-old institution in Pasadena, Calif. It has more than 200 employees, 20,000 square feet of space and the rent to go along with it. In a normal year, it hosts anywhere from 300 to 400 events, bringing in authors for readings and signings, along with customers who buy books and maybe a glass of wine from the bar. But none of that is happening this year.
Like many other stores, Vroman’s is hosting online events to promote new books, which can attract attendees from all over the country but generally bring in almost no money. Last month, it emailed customers, imploring them to come back.
“Our foot traffic and sales are improving, but still down almost 40 percent, which will not keep us in business,” it said. “If Vroman’s is to survive, sales must increase significantly from now through the holidays.”
At McNally Jackson Books, which has four locations in Manhattan and Brooklyn along with two stationery shops, sales are “unimaginably bad,” according to its owner, Sarah McNally. All six shops combined are now bringing in less than its SoHo location would in a typical month.
. . . .
Allison K. Hill, the chief executive of the American Booksellers Association, said the group surveyed its 1,750 members in July and received responses from about 400 of them. Of those who answered, about a third said their sales were down 40 percent or more for the year. But another 26 percent said their sales were flat, or even up. The organization plans to do another survey in January, and Ms. Hill said she expects that positive number to have eroded.
. . . .
Even at stores where sales have held on, profits are often down, Ms. Hill said. In the best of times, the margins at a bookstore are paper thin — traditionally, a successful shop hopes to make 2 percent in profits — but operating during a pandemic is even more expensive.
“We’re working harder for less this year,” said Kelly Estep, one of the owners of Carmichael’s Bookstore in Louisville, Ky.
Mailing a book to a customer requires more time and labor than ringing it up at the register. Some stores are offering hazard pay to their employees or have dedicated a staff member to greet people at the door, making sure they’re wearing masks and sanitizing their hands before they start running their fingers across the books.
. . . .
“If someone told me this time last year I would be spending $20,000 on postage and shipping materials and P.P.E. and extra cleaning for the stores,” said Jamie Fiocco, an owner of Flyleaf Books in Chapel Hill, N.C., and the board president of the American Bookseller Association, she wouldn’t have believed it. “We just didn’t have those line items in our budget, or if we did, they were inconsequential.”
Hanging over all this is the holiday season. Ms. Fiocco said her store does about 30 percent of its business in the last eight weeks of the year, and there are days in December when she sells more in an hour than in a normal day. But this year, customers won’t be able to freely swarm the store at the last minute, so booksellers are trying to encourage early shopping.
Perhaps most worrying is that the supply chain has been under strain. There have been issues with shippers, limited capacity at warehouses and backlogs at printing companies, where books delayed from the spring are running up against releases planned for the fall. Among those is a new memoir by former President Barack Obama, which is scheduled for publication Nov. 17 and expected to be the biggest book of the year.
“There’s a Hail Mary here where the holiday season could really change things,” said Ms. Hill. “To have a book like that come out right at this critical time, it could make a huge difference.”
Many store owners are afraid the printers won’t be able to keep up with demand, or that publishers won’t prioritize indies if supply gets tight, so they’re placing large orders up front for some of the biggest books of the season, like a new cookbook by Yotam Ottolenghi. (Mr. Obama’s book has required other adjustments: At 768 pages, it will weigh 2.5 pounds, said Matt Keliher at Subtext Books in St. Paul, Minn., so the store had to raise shipping fees or else it would lose money on every sale.) Because the demand has been so enormous, Mr. Obama’s publisher Penguin Random House will be sending orders out in batches for stores across the country, from little indies to the big boxes.
“If we could sell 1,000 copies between November 17 and the New Year, that’s going to make a huge difference in us being viable, so we need those books,” said Gayle Shanks, an owner of Changing Hands Bookstore, which has locations in Phoenix and Tempe, Ariz. “We’re really trying to get the message out, to help customers understand that not just for bookstores but local retailers and local restaurants, if they want them to be there when the pandemic over, they have to support those businesses now.”
Link to the rest at The New York Times
From Kirkus Reviews (14 October 2020):
Twenty percent of independent bookstores across the country are in danger of closing, according to a news release from the American Booksellers Association.
Link to the rest at Kirkus Reviews
From The Los Angeles Times (5 October 2020), a piece written by Allison K Hill, President of the American Booksellers Association:
On the side of Vroman’s Bookstore in Pasadena is a mural of a red and black typewriter with a painted piece of paper bearing the words, “I will forever be in love with you. And that’s not fiction.”
When I commissioned this piece in November 2019 as the store’s CEO, it didn’t seem far-fetched to think that Vroman’s, a Pasadena literary institution since 1894, would be around, if not forever, then for a very long time.
Now the store has said it may not make it through the year.
Anyone who has wandered Vroman’s two stories of curated books and gifts, caught up with a friend there for coffee or wine, or met a favorite author at a book signing, knows the shop’s value to the community. But the COVID-19 pandemic has dealt it — and many other beloved independent bookstores across the United States — an unexpected blow.
I left Vroman’s in February to become CEO of American Booksellers Assn. It’s a dream job for me; I love bookstores and I know that Vroman’s and the other 1,745 independent bookstores that we support across the country are heartbeats of their communities. They are run by individuals who love books and are known for their community support, customer service and curation. Recommendations are made by booksellers, not algorithms; displays are inspired by individuals, not corporate planograms.
In my new job I witness on a daily basis what it takes for indies to do this in an industry not known for its financial robustness. As the joke goes: “How do you make a small fortune in the book business? Start with a large fortune.” Independent booksellers are creative, resourceful, hard-working and resilient, and they’ve needed to be during the pandemic.
Since March many independent bookstores have found themselves having to depend on e-commerce and forced to pivot to curbside pickup. They’ve had to replace live events with virtual ones and enforce social distancing, if their stores are open at all. A July American Booksellers’ Assn. survey of 400 member stores found that many have seen sharp sales declines over last year, and results suggest that some 20% of those surveyed may not survive until January 2021.
This statistic mirrors the Small Business Majority’s survey results from August. The group found that, without additional funding, 26% of small-business owners across the United States may not survive past the next three months, and nearly 44% say they may be unable to survive another six months.
If these businesses close, COVID-19 will be listed as the cause of death, but the preexisting condition for many will be Amazon, whose packages have become ubiquitous in apartment building lobbies and on porches across the U.S. Amazon has been boxing out local bookstores and other small businesses all across the country, resulting in the loss of local jobs, local sales tax revenue, and a sense of neighborhood personality, community and tradition. People may not realize the cost and consequences of Amazon’s “convenience” until it’s too late.
. . . .
The COVID-19 crisis has been heartbreaking on so many levels. People have lost loved ones, jobs and businesses. People have lost hope. On a good day I contemplate all the things I’m grateful for, but like all of us there is so much that I miss from my pre-COVID-19 life, particularly browsing the bustling aisles of my favorite bookstores. The Vroman’s announcement was a jolting reminder that on the other side of the crisis we will have lost many of the things we take for granted.
With this realization comes an opportunity for action: Now is the time to create the post-COVID-19 world we want to live in.
Link to the rest at The Los Angeles Times
Digitization Can Support Publishers with Decision-Making
From Publishers Weekly:
“Digitization has made book publishing more efficient.”
According to the “Global Book Publishers Market Report (2021 to 2030): Covid 19 Impact and Recovery,” worldwide sales of e-books are predicted to grow at a compound annual growth rate of 11.7% in the forecast period. This continues a trend that started in 2008 with the introduction of e-reading devices, most prominently Amazon’s Kindle.
Looking at the volume of e-books released each year since 2008, many titles are published directly on self-publishing platforms such as Smashwords or Kindle Direct Publishing. This has created a plethora of new information for traditional publishers—not only about which books are released but also about how individual titles, authors, and entire genres are perceived by readers.
In new research with my colleague Imke Reimers from Northeastern University, we studied how publishers use the information generated through digitization—such as online reviews, detailed bestseller lists, and download figures—to make decisions. Platforms such as Amazon and Goodreads, as well as services such as BookScan or Bookstat, provide new sources of data that can be tapped to make decisions about which authors to work with and which manuscripts to buy.
Using data on almost 50,000 book deals over a period of 12 years starting in the early 2000s, we looked at how digitization has affected the relationships between authors and publishers. In particular, we studied how the advances that authors receive for individual titles or series changed after 2008. As we looked at the data, it became clear that one genre is much more affected by digitization than others: romance and erotica.
No other genre is published as frequently in the e-book format, and no other genre is published as frequently on self-publishing platforms. Likewise, no other genre has seen as many works with a self-publishing background appear on USA Today’s bestseller lists.
So we compared how advances to romance authors changed relative to advances paid to authors who write in other genres. This comparison allowed us to isolate the effect of digitization from other industry trends.
First, we found that advances to romance authors increased by about 20% after the introduction of the Kindle, compared to advances to authors in other genres. We identified two possible explanations for this rise. On the one hand, it might have been driven by a relative improvement of the authors’ bargaining power, given that they now had the option to circumvent traditional publishers and use self-publishing platforms to find their audiences. Alternatively, it could have been driven by an increase in demand for romance books after spectacular hits such as Fifty Shades of Grey.
Secondly, we found that publishers benefitted from the data that became available to them as a result of digitization. To explore this, we took our analysis one step further and asked whether the authors involved in the book deals we reviewed eventually turned out to be successful in the market. This allowed us to study whether publishers’ predictions about manuscripts’ market potential (which we approximate with the size of advances to authors) are accurate.
Strikingly, we found that publishers made relatively fewer errors when choosing manuscripts after the arrival of Kindle, and these improvements are again more substantial for romance authors. This is true for both types of errors: false positives (high advances for manuscripts that eventually flop) and false negatives (low advances for manuscripts that eventually become bestsellers).
In addition, based on regression analyses that estimate whether a book from a deal becomes a bestseller, we found that an advance to a romance author can predict a book’s success at making USA Today’s top 150 bestseller list 33% more accurately, relative to before 2008 and to authors in other genres. This led us to conclude that digitization has made book publishing more efficient.
Finally, we found that publishers that are more likely to invest resources in data analytics (as measured by relevant job postings) see the largest improvements in prediction.
Link to the rest at Publishers Weekly
A Room of My Own
From Writer Unboxed:
I saw a photo of Alix E. Harrow on twitter recently. In it, she’s wearing a baby in a front pack and has a toddler tucked under one armpit, her eyes are glazed — probably from sleep deprivation — and she’s typing madly away. In the caption, she reveals that the manuscript she’s working on will eventually become The Once and Future Witches.
The photo made me nostalgic — I wrote my first book in much the same manner — and it also made me laugh, because–although I cannot fit my almost-adult children on my lap or under my arm anymore, nor would they be caught dead in either position–the search for a private place to write twenty years later is still ongoing.
I had an office in my first house — a loft with a tiny balcony overlooking our yard. The view was so lovely I set my desk against the wall so I wouldn’t be distracted, and I motivated myself with timed breaks on the balcony. The house had an open floor plan, which was perfect for two adults. But babies are much more distracting than views and after our first arrived, my productivity took a dive. Thankfully, we moved to another house soon after. This one had no balcony but did have the benefit of an office for me on the second floor, complete with a door that closed.
The room was large enough to hold a small couch, and often when I was working at night the door would creak open and my toddler would tiptoe in, board book and sippy cup in hand, secure in the knowledge that so long as she was quiet I wouldn’t rat her out to her dad, who had bedtime duty. I stocked the bookshelves, not just with craft tomes, but also with stuffed animals and quiet toys, and I painted the walls kid-friendly pastels. I wrote for newspapers and magazines in that room, and finished and sold my first novel from there.
But as time passed, the kids grew up and went to school. I no longer needed to barricade myself in to finish an article or chapter, no longer had to work only during nights and nap times. Oddly, now that I had what I’d longed for — a few uninterrupted hours of writing time — the office felt far too quiet. I took to wandering the house with my laptop, writing some days at the kitchen table, other times on the living room couch. When I truly felt like I was going crazy in the silence, I packed up and headed to a local library or coffee shop.
And then Covid struck. Like most everyone else, all my chickies came home to roost at once, filling the house. The two teenagers stayed mostly in their bedrooms, which left my husband. Who needed a place to work with a door that closed. A place like … my office.
On paper it made sense. He has a job that often involves discussing confidential information, whereas most of my conversations take place with people I’ve made up in my head. Even so, he was reluctant to settle in, convinced things would soon be back to normal. But as one month turned into two, then four, my beloved toys and artwork got relegated to corners where they wouldn’t show up on corporate Zoom meetings. Coffee cups and button-downs replaced tea cups and cardigans, and the aroma of lavender and scented candles no longer lingered.
My husband offered to carve out a corner for himself in the basement or the bedroom, but neither of those solutions were practical given his working hours. And even if he found space elsewhere, I wasn’t sure I wanted to go back to my office. I’m not a big believer in cosmic energy, but I could feel that the room wasn’t the same. Instead of my cozy nest, it now had a corporate feel, and it would take more than rehanging some art to change the vibe.
So instead, once again I became a nomad, carting my laptop and bag of files and notes from room to room. The kitchen table worked until lunchtime, when my fellow inmates needed to eat and couldn’t understand why I was surly about stopping my writing mid-sentence. The bedroom made me sleepy. The basement was quiet, but the lack of natural light made me irritable. The porch worked well on days when the weather cooperated and there were no mosquitoes, which meant about once a week. During the first surge, coffeeshops and libraries were out of the question.
Link to the rest at Writer Unboxed
Subscriber List Cleaning
PG did a bit of cleaning of the subscriber list for TPV after filtering through a bunch of comments that were clearly spam that sneaked past the TPV spam plugin.
This included consulting a list of internet country codes known for generating lots of spam.
He noted one domain on the list - bunkbedsforsale.com and a lot of Gmail addresses that looked something like girls.x.4.d.g.9.0.8.1.c.z.sex.y.b.3@gmail.com.
If you’ve been improperly cleaned, sign up to subscribe to the daily TPV email again.
It’s more fun
It’s more fun to be a pirate than to join the navy.
Steve Jobs.
I am sorry to see you here
I am sorry to see you here, but if you had fought like a man, you needn’t be hanged like a dog.
Anne Bonny
As to hanging
As to hanging, it is no great hardship. For were it not for that, every cowardly fellow would turn pirate and so unfit the sea, that men of courage must starve.
Anne Bonny
Spies, Lies, and Algorithms
From The Wall Street Journal:
Computers have transformed many institutions and professions in the 21st century, and the world of espionage especially. In “Spies, Lies, and Algorithms,” Amy Zegart, a Stanford professor of political science and an occasional consultant to intelligence agencies, has provided a lucid and sobering account of how digital and other technological breakthroughs are “generating new uncertainties and empowering new adversaries” for the United States at a time when its intelligence agencies are uniquely stressed.
Ms. Zegart opens her book with a survey of the nation’s rapidly changing “threat landscape” (Russia, China, terrorist groups); the sudden arrival of “open-source intelligence” (live-streaming amateur videos, time-stamped Twitter and Facebook posts); the consequently high volume of internet data relevant to intelligence; and the challenge to the U.S. intelligence community of keeping up with it all. Her aim is to give the general reader a non-Hollywood understanding of 21st-century intelligence as well as the daunting challenges that American spy agencies now confront.
The U.S. intelligence community, outlined concisely by Ms. Zegart, is composed of 18 separate organizations, including two independent agencies: the Office of the Director of National Intelligence, which oversees operations, and the Central Intelligence Agency, which runs spies and engages in covert action. There are nine Defense Department elements, including the National Security Agency, which makes and breaks code; the National Reconnaissance Office, which develops and deploys spy satellites; and the intelligence offices of the various armed forces. The other seven elements include divisions of the Department of Homeland Security, the Drug Enforcement Administration, the FBI and other government entities. Ms. Zegart catalogs the difficulties of coordinating these disparate organizations, each with its own culture and skill set and priorities.
As the world has become more and more connected electronically, so much data is now online—Ms. Zegart estimates that 80% of what the intelligence community gathers comes from publicly available sources—that intelligence agencies are losing their traditional advantages to nongovernmental actors. Spy satellites and high-resolution cameras mounted on military aircraft, once the exclusive preserve of the government, now have rivals in small commercial satellites that can observe even license plates from space. Costs for users have plummeted; Google Earth is free. A “cottage industry of non-governmental nuclear intelligence collectors and analysts” who track nuclear efforts in North Korea and Iran has emerged, along with such phenomena as the Netherlands-based Bellingcat, a private community of journalists and researchers that has provided remarkable information about the secret Russian unit that has attempted to assassinate dissidents in Europe.
While there are obvious benefits to such activities, the privatization of intelligence also has costs and dangers. Ms. Zegart is at her best when describing cyber threats. “In many ways,” she writes, “cyberspace is the ultimate cloak-and-dagger battleground, where nefarious actors employ deception, subterfuge, and advanced technology for theft, espionage, information warfare, and more.” Enemy states and terrorist groups are “hacking both machines and minds,” not only within American institutions but in our living rooms. “Artificial intelligence is creating deepfake video, audio, and photographs so real, their inauthenticity may be impossible to detect. No set of threats has changed so fast and demanded so much from intelligence.”
. . . .
The anonymity of the internet combined with the widespread use of secure encryption has led to increasingly vitriolic and often hard-to-refute false claims clogging all channels of communication. Private technology companies like Google, Amazon and Facebook, incentivized to pursue profits and operating on a global scale, are often reluctant to surrender their users’ privacy even when democratic governments assert national-security claims. While China and other repressive regimes employ facial recognition software to harass, intimidate and imprison entire populations, many American Googlers have protested any cooperation by their employer with the American intelligence community.
The United States and other technologically advanced countries are increasingly vulnerable to large-scale cyberattacks that can corrupt data or compromise sensitive infrastructure. In 2015 a Chinese intrusion stole 21 million security-clearance records from the U.S. Office of Personnel Management; in 2020 Russia obtained access to several American nuclear labs, government departments and Fortune 500 companies.
Link to the rest at The Wall Street Journal (PG apologizes for the paywall, but hasn’t figured out a way around it.)
How To Get Your Self-Published Book Into Libraries
From The Creative Penn:
If you haven’t considered libraries as a market for your self-published book(s), you should.
Why? For one, there are 2.6 million libraries globally1, and they spend roughly $31 billion annually2! In the U.S., library expenditures are $14.2 billion a year2, and of this amount, $1.4 billion1 or 10.2% is spent on books!
Secondarily, the library market is growing! Two years after Joanna posted my original article, How To Get Your Book Into Libraries, the number of Academic Libraries worldwide grew to 95,361, a 111.8% increase, and Public Libraries globally grew to 406,834, a 39.4% increase! In the U.S., the number of Academic Libraries had grown 12.5%, and there were 90.5% more Public Libraries!
And third, libraries are purchasing more eBooks. According to the American Library Association (ALA), in 2020, OverDrive (a provider of eBooks to Libraries) loaned out more than 289 million eBooks worldwide, a 40 percent increase from 2019, a shift the company attributed to the global pandemic.
. . . .
If you wonder if libraries buy self-published books, the answer is, “Yes, they do.”
In its April 5, 2021 article, How Library Distribution Works for Indie Authors, the Alliance for Independent Authors (ALLI) shared the results of a 2016 survey conducted by US-based publishing service New Shelves. Per the survey, “… 92 percent of librarians reported that they regularly purchase from self-published authors and small presses.”
Although there still may be some libraries whose Collection Development Policy (the guidelines libraries use when making book purchasing decisions) might state they don’t buy self-published books, those excluding are becoming rarer and rarer.
I believe my situation is a good example. As of this writing, 156 libraries worldwide have acquired 192 copies of my self-published titles since I first introduced them to librarians a few years ago.
Also, in the last two years, I haven’t had one library inform me they don’t buy self-published books. And if you’ve heard that it’s hard getting a self-published book into a library, I would say, “It shouldn’t be easy because of the vital role libraries play in societies, but I and others are proof that it can be done.”
Link to the rest at The Creative Penn
Who Are You Writing For?
From Writer Unboxed:
What do I, as an author, owe to myself? What do I owe to my publisher? To my readers?
I think about this often as I promote my debut novel, Waiting for the Night Song, while simultaneously revising my forthcoming novel, The Last Beekeeper, and drafting what will hopefully become my third novel.
To whom do I owe what?
I wrote Waiting for the Night Song with no expectations. I created a story I needed to tell, not knowing if I would ever sell it. I wrote the book for myself. After landing the elusive book contract, I incorporated changes based on suggestions from my editor. At this point, I was still writing for myself — sort of.
New expectations started lining up.
I wanted to please my editor and my agent, both of whom took a gamble when they signed me. I wanted to make them proud. I wanted my book to succeed commercially. But mostly, I need this book of my heart to be mine, to be the book I had envisioned for so many years.
It was still my book, right?
Ideas, many of them bad, started sneaking into my head. Should I add more surprise twists? Books with twisty plots were topping the charts, so I added a poorly-conceived plot contortion, for no reason other than I thought readers wanted it.
I quickly deleted the ridiculous subplot because it didn’t serve the theme of my book, and this book was, after all, for me.
To be clear, my editor and agent have never pressured me to change my writing in ways that didn’t feel right for my story. They make suggestions, not demands. But after years of writing just for myself, I now feel the burden of writing for other people, as well.
I started to wonder: Was Waiting for the Night Song still mine?
Link to the rest at Writer Unboxed
A monk in 14th-century Italy wrote about the Americas
From The Economist:
That vikings crossed the Atlantic long before Christopher Columbus is well established. Their sagas told of expeditions to the coast of today’s Canada: to Helluland, which scholars have identified as Baffin Island or Labrador; Markland (Labrador or Newfoundland) and Vinland (Newfoundland or a territory farther south). In 1960 the remains of Norse buildings were found on Newfoundland.
But there was no evidence to prove that anyone outside northern Europe had heard of America until Columbus’s voyage in 1492. Until now. A paper for the academic journal Terrae Incognitae by Paolo Chiesa, a professor of Medieval Latin Literature at Milan University, reveals that an Italian monk referred to the continent in a book he wrote in the early 14th century. Setting aside the scholarly reserve that otherwise characterises his monograph, Mr Chiesa describes the mention of Markland (Latinised to Marckalada) as “astonishing”.
In 2015 Mr Chiesa traced to a private collection in New York the only known copy of the Cronica universalis, originally written by a Dominican, Galvano Fiamma, between around 1339 and 1345. The book once belonged to the library of the basilica of Sant’Ambrogio in Milan. In Napoleonic times, the monastery was suppressed and its contents scattered. The owner of the Cronica let Mr Chiesa photograph the entire book and, on his return to Milan, the professor gave the photographs to his graduate students to transcribe. Towards the end of the project one of the students, Giulia Greco, found a passage in which Galvano, after describing Iceland and Greenland, writes: “Farther westwards there is another land, named Marckalada, where giants live; in this land, there are buildings with such huge slabs of stone that nobody could build them, except huge giants. There are also green trees, animals and a great quantity of birds.”
Mr Chiesa says that giants were a standard embellishment of faraway places in Norse folklore and, indeed, Galvano cautioned that “no sailor was ever able to know anything for sure about this land or about its features.” The Dominican was scrupulous in citing his sources. Most were literary. But, unusually, he ascribed his description of Marckalada to the oral testimony of “sailors who frequent the seas of Denmark and Norway”.
Mr Chiesa believes their accounts were probably passed on to Galvano by seafarers in Genoa.
. . . .
[I]t could help explain why Columbus, a Genoese, was prepared to set off across what most contemporaries considered a landless void.
Link to the rest at The Economist
College Student Views on Free Expression and Campus Speech 2022
From The Knight Foundation:
College campuses have long been places where the limits of free expression are debated and tested. In recent years, this dialogue has grown more fraught as some schools have sought to create a more protective speech environment for students. Moreover, key events shaping the past two years, such as the COVID-19 pandemic, the racial justice movement and the 2020 election, have only added deeper dimensions to the dialogue around free speech playing out on campus and in society at large.
The “Knight-Ipsos College Student Views on Free Expression and Campus Speech” report is the fourth in a series of Knight Foundation reports measuring college student attitudes toward speech and the First Amendment since 2016.
. . . .
KEY FINDINGS
- Students view speech rights as important, yet less secure than in years past: Students continue to believe First Amendment rights and concepts of free speech are important to democracy. However, the percentage of students saying speech rights are secure has fallen every year since this question was first asked in 2016. This includes a 12-point decrease from 2019 as an increasing number of students—particularly Republicans—say they believe speech rights are threatened.
- Students of color believe their speech is less protected: While a majority of college students express confidence that the First Amendment protects “people like them,” Black students in particular feel much less protected, with a sharp decline from 2019 to 2021.
- Students believe exposure to a wide spectrum of speech at college is important: Most students continue to say colleges should allow students to be exposed to all types of speech, including political speech that is offensive or biased, rather than prohibiting speech they may find offensive.
- Students favor college policies that limit racist speech, but support for other speech interventions remains low: Most students favor colleges instituting policies that restrict the use of racial slurs on campus, suggesting that, for them, this particular category of speech does not merit mandated exposure on campus. Just 1 in 4 students favor schools disinviting controversial speakers, down from more than 2 in 5 in 2019. Similarly, the number of students who support colleges providing safe spaces or speech codes has fallen over the past two years.
- Students say the campus climate stifles free expression, yet speech on campus is making nearly 1 in 5 feel unsafe: More students now say the climate at school prevents some from saying things others might find offensive, and fewer feel comfortable disagreeing in class. Yet slightly more now report feeling unsafe because of comments made on campus than in 2019. This is particularly true for female students and students of color.
Link to the rest at The Knight Foundation, where you can find a lot more information on the topic and download a 44-page PDF report about the survey results.
China isn’t our only intellectual piracy problem
From The Deseret News:
The U.S. economy runs on startups. For all of America’s brand-name mega-corporations, it’s young firms that create most of our new jobs during periods of economic growth.
Those startups, in turn, depend on America’s famously strong laws protecting their patented inventions and other intellectual property. The only way someone with a big idea but minimal resources can outcompete established firms is through proper government protection of their innovations.
Today, we are failing in that responsibility. Instead, our laxity is empowering predators foreign and domestic — endangering not only the next Apple, Microsoft, or Facebook, but our entire economy.
For years, the greatest threat to American intellectual property has been China. As our economy became more globalized and digitized, Chinese IP piracy became endemic — totaling an estimated $600 billion in costs to the U.S. economy per year. In 2019, a CNBC survey of American corporations found that nearly one-third of respondents had experienced IP theft by Chinese pirates in the past decade. Testifying before Congress in 2020, Facebook CEO Mark Zuckerberg said, “I think it’s well documented that the Chinese government steals technology from American companies.”
More telling than Zuckerberg’s acknowledgment, however, was the strange but unmistakable equivocation by the other Big Tech executives at the hearing. When asked the same question, the CEOs of Apple, Amazon and Google — individuals famous for their breadth of knowledge and laser focus on their businesses — all shrugged and testified only that they hadn’t personally seen any Chinese IP piracy.
While many, including the U.S. Attorney General, slammed them for “kowtowing” to Beijing, there is another reason those firms might not want to shine too bright a light on IP theft: it’s become a valuable part of their own business models.
. . . .
Early this month, the U.S. International Trade Commission issued a final ruling finding that Google infringed on five patents belonging to Sonos, a company that makes smart speakers. The story is a worst-case scenario for a startup innovator. Over a decade ago, Sonos developed one of the most advanced wireless audio systems in the market — a product so impressive that Google wanted to partner with the company on it. Sonos alleges that early in the partnership, Google lifted Sonos-patented technology for Google’s own audio equipment — and continued doing so for future products despite Sonos calling the tech giant out for infringement.
Sonos’s experience was no fluke. Google faced 48 patent infringement lawsuits in 2021.
That’s more than any other company, but Google is certainly not the only alleged perpetrator.
Sonos has accused Amazon of stealing the same technologies for use in its Echo audio systems. Additionally, in 2020, a federal jury ordered Amazon to pay $5 million to Texas-based Vocalife for infringing on its patents to make Echo. Meanwhile, Apple was recently ordered to pay $300 million in damages to Optis Wireless Technology for patent infringement.
It’s no accident, then, that the number of IP lawsuits rose in 2020 for the first time since 2015, and court awards rose to $4.67 billion from just $1.5 billion in 2019.
It also makes holding China to account much harder. After all, if the richest and most powerful businesses in America are ignoring our intellectual property laws — supposedly some of the strongest in the world — why shouldn’t our global adversaries?
The real issue here isn’t complicated: When laws against theft aren’t vigorously enforced, thieves are going to steal. That’s true as much for sophisticated IP infringement as it is for the wave of organized shoplifting in California today. With billions of dollars at stake, slaps on the wrist or gentle nudges aren’t going to deter highly motivated pickpockets in Beijing, Silicon Valley, or anywhere else. Congress has to tighten up our IP laws and stiffen penalties, and the Justice Department needs to ramp up enforcement while there are still innovative American startups left to save.
Link to the rest at The Deseret News
PG says authors shouldn’t rest easy because the OP talks about patents instead of copyrights. Ebook piracy is at a significant level. Overpricing of ebooks by traditional publishing is certainly a motivation, but pirates aren’t known for staying away from indie authors as well.
When a friend talks about a great new website where all sorts of ebooks are marked way down from the prices Amazon charges, don’t hesitate to explain that it’s likely a pirate site. In addition to preventing authors from being paid for their works, piracy destinations are also known as great places to get your computer or tablet infected with malware. Then, it’s possible your friend will share the malware with all of her friends as well.
If you have to trash a computer or even a hard drive due to malware, a new one will cost you much more than any number of ebooks would have on Amazon. If you have to hire someone to come in to remove the malware, that’s also going to cost a lot of money. If you lose all your tax information or your manuscripts, that’s another potentially expensive consequence. If your friends get infected from your computer and have to spend money cleaning up their problems, you may not get invited out to lunch in the future.
And if you find a copy of a NYT bestseller that usually costs $19.95 that only costs 99 cents, conveniently payable by credit card, you may find your life gets a lot more complicated as well. Think of how your significant other will respond to $5,000 in new charges on your joint credit card.
Yes, you may be able to get some or all charges reversed, but, depending on the circumstances, you may not. At a minimum, you’re going to have to spend a lot of time explaining to some suspicious credit card employees how you were so stupid as to fall for a well-known scam.
To be clear, PG isn’t saying that every pirate site for free ebooks is infected with malware, but enough are that it’s a good idea to stay away from all of them because the potential for an expensive loss is greater than any money you might save in the short run. Besides, cheating authors whose books you like is really low.
Pulling back to a longer philosophic perspective, PG has learned that life will be more pleasant and easier for a person who doesn’t act like a jerk.
An Excerpt from “We Are All Whalers”
From The University of Chicago Press blog:
Recently, I spent an early April day in the southwestern corner of Cape Cod Bay, in eastern Massachusetts, in the United States, with a friend. He had been at sea his entire working life, but had never knowingly been close to a right whale. His day job was master of an oil tanker on the Valdez, Alaska, to San Francisco, California, run, where he might have been close to a North Pacific right whale (Eubalaena japonica).
He was vastly overqualified to skipper our boat, which he did while I piloted a small drone to measure the lengths and widths of the many feeding North Atlantic right whales (Eubalaena glacialis) we had found in a small area. There was no wind that day. The sea was like a millpond. It was crisp, cold, sunny, and quiet. We shut down the motor, drifted, watched, and listened. As each animal surfaced, exhaled, and immediately inhaled, we listened to the unique cadence of their breaths, and we watched their steady progress through the water with their mouths wide open, filtering the clouds of food close to the surface.
Periodically, they slowly closed in on the boat, and we could see into their open mouths, with small eddies of water peeling away from their lips. Much larger eddies formed in their wakes as their powerful tails and bodies pushed them along. They made tight turns, using their huge flippers and tails as rudders, to keep themselves within the food patches.
This went on all day. As the sun started to sink behind the cliffs on the nearby western shore of Cape Cod Bay, their creamy white upper jaws, just visible above the surface, turned to a vibrant golden hue. It was a peaceful, majestic, timeless sight, and a huge privilege to be permitted to study these animals.
At the end of the day, my friend said that he understood why I care so passionately for them. Words often fail when I try to express the awe and wonder that these animals elicit; this book is my attempt to do them justice, and keep them out of jeopardy.
My hope is to convince you that the welfare of individual North Atlantic right whales, and the very survival of the species, is in our hands. Few humans eat whale meat anymore, but fishing techniques unintentionally harm and kill whales. Even vegetarians contribute to the problem, as we all benefit from global shipping of consumer goods and fuel, which, in its current iteration, leads to fatal collisions with whales. Entanglement in fishing gear can sentence these animals to months of pain and a slow death.
Both the US and Canadian governments are stuck in a major conflict of interest: protecting the livelihoods and businesses of the marine transportation and fishing industries, but at the same time recognizing the value of biodiversity, animal welfare, and avoidance of species extinction. Recently, the latter values have taken a back seat. It doesn’t have to be this way. We have the technology and the collaborations that are necessary to change the right whales’ future, but consumers have to use their wallets to make it happen. Hopefully, politicians still listen to their electorate.
. . . .
This is a story that began for me as a child in England, raised by caring people, learning from our challenges and traumas, as all families do. I was taught how to survive on the water, maintain boats, and explore. I trained as a veterinarian, but I also had the chance to pursue my own curiosity. I was shown the enormous wealth of a productive marine ecosystem, off eastern Newfoundland, but also the harsh reality of the trauma whales face when in conflict with humans harvesting a mutual food resource. An opportunity arose to document the remarkable efficacy of direct harvest of large whales in Iceland—a reality whose relevance to my later work took decades to come in to focus.
I then describe a small window I was given into the millennia of native subsistence harvest of the bowhead whale in the Arctic. The native hunters had truly conserved the whales’ habitat, and hence the whales, in spite of the best efforts of both nineteenth-century commercial whalers from New England to wipe out the species and recent oil exploration to degrade its habitat. The Alaskan Iñupiaq sense of the long view, and respect for the whales as a part of their culture, made me hope that modern marine industries could also sustainably coexist with right whales in their habitat.
As I slowly grew to understand the impacts of industrial fishing practices and vessel collisions on large whales, I fell into the role of a large whale trauma diagnostician. Along with a few dear colleagues, I provided a scorecard for government efforts aimed at reducing such impacts. We worked with all of the affected whale species in New England: humpback, blue, fin, sperm, minke, and right, in addition to smaller whales, dolphins, and seals.
But it was the right whales that were the most prominent and imperiled in their plight. But what is good for right whales will be good for the others, too. We tried to intervene with some sick whales, to reduce their suffering, but realized that prevention of the trauma was the only lasting solution. So now I work with scientists, engineers, fishermen, lawyers, government managers, and nongovernmental organizations to promote a safe, profitable, sustainable seafood harvest that will allow the North Atlantic right whale to turn another corner and prosper once more. Despite all I’ve seen, I have hope. I believe we can reverse the trend such that a thousand years hence, right whales will be as numerous as before we started killing them, whether with intent or by accident.
Link to the rest at The University of Chicago Press blog (paragraph breaks added to assist in online reading)
This Review Should Not Exist
From Public Books:
This review should not exist. I should not write it.
Pieces like this one always carry the same heading: “Dispatches from [insert country/geographic region],” “Three recent novels from [insert identity/language/culture].” If “natives” like me write these pieces, we acquire the voice of “our” culture and speak for its history. If others—nonlocals and, perhaps, nonspecialists—write them, historical specificity can evaporate into belles-lettristic formalism or stereotype, apolitical and stale. Such essays are, nevertheless, irrefutably important, since they can help bring foreign writers to US audiences. When well-written, they have the potential to rewrite harmful and boring tropes and offer new ways of pondering the literary landscape. Just like novels, though, they often uncritically fulfill the market’s demands (as I might be doing here).
The tangled incentives motivating this essay include: monetary and career incentives that led me to emigrate to and study in the US; monetary and career incentives that make translation into English essential for Third World writers (especially Latin American ones); and this publication’s platform—people interested mainly in American and British literature, with advanced humanities degrees conferred by US universities. Essays like this one risk calcifying the imperial dynamics that inevitably produce them, relegating the literary and cultural works they promote to the lesser literary field of keyword-laden generalities.
“Latin America” is one such keyword and, nowadays, a gringo fabrication. Even if I could rescue something decidedly autochthonous and pure that unified the region, I wouldn’t know how to tell it apart from the Yankee, imperial mythology. Latin American authors engaging elements of the continent’s shared canon and interconnected histories face a double bind that demands, in a sense, that they establish a relationship with “Latin America” as a formulation emanating from above—from centers of literary power, nowadays New York and formerly Paris—to be translated, to sell, to make money from their literature. Latin America registers in those literary centers as an aggregation of tropes established mostly by the aesthetics of token authors inducted into the “global” literary canon—Neruda, García Márquez, and Bolaño key among them. Borges, for these readers and critics, might as well have been French.
Obviously, economic and institutional rewards come to those willing to pander to US desires (just ask Isabel Allende). At the same time, one cannot deny that authors’ dependency on the US book market has increased exponentially in recent years. This has itself become a literary theme. Three recently translated, very different novels—César Aira’s The Divorce, Dolores Reyes’s Eartheater, and Pedro Mairal’s The Woman from Uruguay—each illuminate and interrogate aspects of top-down, imperial representational demands. At times critical of and dexterous in playing with gringo expectations, these novels attempt to develop forms of literary imagination, of reading and writing, that elude instead of rehearsing a partially gringo-defined, essential Latin Americanness.
. . . .
César Aira’s The Divorce was originally published in 2010 and comes to English courtesy of New Directions, translated by Chris Andrews and prefaced by Patti Smith. The novel assumes the voice of a wealthy, educated resident of Providence, Rhode Island (a Brown professor?), who moves, almost on a whim, to a Buenos Aires hostel following a painful divorce. “A temporary withdrawal on my part would be the kindest thing, for me and for my daughter,” he explains. “When I returned, all smiles and gifts, we would reestablish our relationship on the terms laid down by the judge.” Perhaps escape can quell the agonies of separation.
Latin America is ideal for fleeing, since it has historically been cast as exterior to history: a location in permanent, nondialectical détente. Think of Burroughs fleeing to Mexico after committing murder; Hemingway’s long love affair with La Finca Vigía; Britons awed by Patagonia. Atemporality draws imperialists like flies.
Likewise, for Aira’s narrator, Buenos Aires is a pause, unimportant and nonnarrative in his life because what matters is the “Providence (Rhode Island)” timeline. That name itself assumes an ironic guise, mocking gringo self-regard and foreshadowing the narrative’s distaste for P/providence.
Upon arriving in Buenos Aires, the narrator journeys to a local coffee shop. He witnesses a young man get drenched by the accumulated water of a retracting awning. Everything stops. As our narrator stares on, the soaked Enrique recognizes Leticia, the childhood acquaintance he was originally on his way to meet. A remarkable subnarrative arises here—“They hadn’t seen each other since the day they met, which was also the day that had marked the end of their childhood”—as Aira leads us down the story of Enrique and Leticia’s elementary school. That institution had burned down in a demonic fire they escaped by entering an also burning miniature model of the school that they found in a basement. This aside concludes with Enrique and Leticia’s reduction to atoms, which then escape the school together with millions of similarly sized priests.
. . . .
Aira does not really engage the more tangible historicity of Buenos Aires and Argentina, because his story mostly operates on a metafictional level. Meanwhile, Eartheater, Dolores Reyes’s first novel (translated by Julia Sanches) does tussle with the city’s specific pasts and presents.
Reyes narrates the story of an unnamed young woman from a Buenos Aires slum who sees her father murder her mother, then feels an uncanny urge to devour earth at her family’s property. Doing so, she briefly relives the moment of the killing. The narrator quickly realizes that by eating dirt from a specific location, she can witness the horrible events that transpired there. Quickly, albeit guiltily, she monetizes the skill, transforming into a sort of detective. Most of her clients are grieving parents looking for children, mainly daughters murdered by men—their partners and fathers. She hesitantly begins dating a policeman, whom she later encounters working at the scene of her ex’s murder, at a club she attends with her brother and his friends on the same night as the killing. Her ex’s murderer almost kills them, too, until her missing father reappears, saves them by stabbing their assailant, and vanishes into the night.
Eartheater gestures towards the vernacular of Buenos Aires villas (or slums), and Julia Sanches’s translation conveys that unique prosody remarkably well, despite some shaky moments. Mirroring the narrator’s mystical ability, the narrative hugs its haunted ground; land and earth document a history that the state does not. This is particularly the case in Argentina, where the aristocracy has historically hoarded and abandoned vast swaths of land, creating massive latifundios populated by poor, exploited workers who inherit the conditions and destitution of slaves.
Such land is increasingly owned by transnational corporations unconcerned with environmental and social destruction. These same heinous corporations probably produce the beer and junk that the narrator constantly devours. Her rate of consumption makes her inexplicable relationship with dirt feel almost satirical, as if Reyes were ironically refracting the deficient diet of the Argentine poor by suggesting that they eat the material base of their condition: land itself. Maybe then something will change.
At the novel’s very beginning, the narrator says, “Mamá stays here. In my house. In the earth.” Our narrator struggles to preserve her murdered mother’s proximity so that the latter’s life might not be forgotten, so that justice might remain possible, because dirt ties her to the absent. The traces of brutality that infect daily life can only be interpreted (literally) from below; her cop boyfriend cannot understand the violent histories that envelop the narrator, her family, and her friends. He reduces those subject to such histories to otherness by insulting them, calling them “estos negros.” Sanches’s use of “scum” here fails to fully relay the racialized connotations of the Spanish (literally, “those blacks”).
In Eartheater, locality—determined by the dirt the central character eats, the ground she walks—is the only true solution to the cycle of violence. Even so, Reyes does not offer a neat tale of redemption. The narrative ends when the femicidal father returns to save the main character’s life, and she says: “Twice I’d seen my old man kill.” The two killings were undeniably different—opposed, even—but murder nonetheless. The narrator’s departure, her flight from the neighborhood, interrupts but does not definitively end this cycle. Violence continues, and Reyes reminds us that individuals, no matter their gifts or nobility, cannot modify structures when acting alone.
If Aira undoes the legend of Argentina as a leisurely Eden, then Reyes does so twice over, turning Buenos Aires into a grim inferno of destruction and treason. An uncomfortable history comfortably forgotten undermines yet again whatever pastoral sense of benevolent calm existed in the US conception of Latin America.
Link to the rest at Public Books
PG is not an expert on the subject, but his observation (which may be unfair or incorrect in whole or in part) is that, according to the accounts PG has read in recent years, many second and third-world nations share some similar characteristics.
- They are either currently governed by dictatorships or have a 20th Century history of being governed by dictatorships with any sort of democracy being new and less-than-perfect.
- Often, outsiders (beneficiaries of colonial power or capitalists exploiting local individuals or resources) are blamed either explicitly or implicitly for some or all of the problems in their societies and governance.
- Living standards are lower than in first-world countries and writers portraying these countries either blame western/colonial history for current problems or otherwise show resentment toward individuals or groups that have had the benefits that accompany residence in first-world countries AKA “the rich” or “those who are richer than most in my country”.
PG understands that he has lived his life in what some regard as the most-heinous of Western Exploitational Nations, the United States.
However, to the best of PG’s knowledge, he has never personally benefitted from the exploitation that took place in any second or third-world nation. Neither he nor any member of his family of origin inherited any wealth or power. PG knows a lot about his ancestors and doesn’t think any of them had inherited wealth or oppressed the American Indians or others in this nation or in their nations of origin.
Prior to settling in the United States, none of PG’s ancestors were wealthy by the standards of their day and place. None were rulers of anything outside of their home and small land holdings. On one line, some male ancestors attended one of the colleges at Oxford, but it was for the purpose of becoming ministers which is what they did after they finished their studies. Then, as now, earning a living as a minister is not one of the better ways to become rich and pass riches down to your children.
Nobody killed any Native Americans. Some of PG’s ancestors were, however, killed by Native Americans.
Any money that existed in PG’s family of origin in the Twentieth Century was earned, not inherited and disappeared in the Great Depression. Nothing tangible was inherited by PG’s parents (who are both deceased after lives spent working hard to support their family, including PG).
From his family of origin, PG inherited a Protestant work ethic and, from his mother, a degree of intelligence.
Prior to college, PG attended either isolated country schools in the American West or typical midwestern small-town schools. Less than 10% of PG’s graduating class in high school finished college. Less than 20% tried to go to college.
With the help of large scholarships, student loans and working 15-40 hours per week while he was in college, PG graduated from what many would characterize as a good school. That helped him get a good job when he graduated and, eventually, to attend law school.
To the best of his knowledge, neither PG nor any member of PG’s family going back a long way has ever exploited anyone of a different race or ethnic origin for any purpose. Definitely nobody got rich doing so. Most definitely, PG has never inherited anything tangible from his ancestors. He did inherit a work ethic and a tradition of attending church, each of which he values.
Thus, PG has never felt any white guilt or guilt for being an American or sense that he owes a particular ethnic group any recompense or help other than general Christian charity towards those who have less than he has regardless of their race or ethnic origin.
If you truly love film
If you truly love film, I think the healthiest thing to do is not read books on the subject. I prefer the glossy film magazines with their big color photos and gossip columns, or the National Enquirer. Such vulgarity is healthy and safe.
Werner Herzog
Artists use frauds
Artists use frauds to make human beings seem more wonderful than they really are. Dancers show us human beings who move much more gracefully than human beings really move. Films and books and plays show us people talking much more entertainingly than people really talk, make paltry human enterprises seem important. Singers and musicians show us human beings making sounds far more lovely than human beings really make. Architects give us temples in which something marvelous is obviously going on. Actually, practically nothing is going on
Kurt Vonnegut
Having your book turned into a movie
Having your book turned into a movie is like seeing your oxen turned into bouillon cubes.
John le Carre
Film Adaptations Of Books Earn 53% More At The Worldwide Box Office
From Forbes (2018):
Film adaptations of books gross 44% more at the U.K. box office and a full 53% more worldwide than films from original screenplays, according to research commissioned by the Publishers Association and produced by Frontier Economics.
The report also found that 43% of the top 20 highest-grossing films in the U.K. from 2007 to 2016 were book-based and another 9% were based on comic books. Data for the report was compiled from a variety of sources, publishing industry magazine The Bookseller notes, incorporating case studies and publically available information alongside contributions from the BBC, UK Theatre and Nielsen BookScan.
“In short, published material is the basis of 52% of top U.K. films in the last 10 years, and accounts for an even higher share of revenue from these leading performers, at 61% of U.K. box office gross and 65% of worldwide gross,” says the report, adding later that “Across any of the common measures of viewership, book adaptations on average outperform shows based on original scripts or on comic books and other sources.”
Link to the rest at Forbes
Demand for TV rights ‘never been higher’
From The Bookseller:
In an overcrowded market with the proliferation of streaming platforms alongside the traditional broadcaster, creating content based on previous IP is an ever-growing trend . . . Not that it wasn’t a trend before, it’s just that IP generation (writing a book, creating a podcast, a YouTube series) has never been as accessible or opportunity-filled as it is today. Books still have the lion’s share of the source material market for TV and cinema adaptation. But not all books are created equal when it comes to adaptability.
Some genres are more easily transferrable to the screen and tend to create a better connection between the source audience and the series viewers. Classics of world literature still retain the trophy when it comes to literary adaptations.
Across genres, from Jane Austen to Bram Stoker, these stories have been revisited time and time again in the visual medium, allowing younger generations to discover them anew.
Every time a new “Dracula”, a new “Pride and Prejudice”, a new “Frankenstein” or “Sherlock” hit the screen, the original texts are looked at with fresh eyes, as curiosity around the source material is reinvigorated, and audiences revisit the original books to discover those nuances that can only exist in the written form. It is definitely true that you can make one book from a series, but a thousand series from a book.
When it comes to new titles, thrillers reliably make promising adaptation fuel. The booming of new authors in the thriller space and the insatiable global appetite for crime stories that has always characterized fans of television series are a match made in heaven. From the most established and well-recognised IP to the newcomers, content providers have always been eager to turn a “page-turner” into a bingeable series. From HBO’s “Sharp Objects” (Gillian Flynn) or “Big Little Lies” (Liane Moriarty), to “The Haunting of Hill House” (Shirley Jackson), from “Hannibal” (Thomas Harris) to “The Alienist” (Caleb Carr), watching a series based on a thriller novel has never been so satisfying.
Fantasy, however, is probably the genre that benefits the most when it comes to screen adaptation. From the gothic saga of “The Originals” to the modern tale of “Discovery of Witches”, from the epic battles of “Game of Thrones” to the generational conflicts of “His Dark Materials, thanks to the evolving world of CGI and special effects, it’s become increasingly possible to bring to life with staggering precision and realism the worlds we imagined in the page. But the bigger the book, the bigger the responsibility of those who adapt it: for if a book has managed to captivate thousands of fans around the world, one needs to be very cautious and respectful when it comes to translating onto the screen, so as not to lose the connection that the readers have with the original story. It also of course comes with the unique opportunity of attracting a completely new pool of fans, and producers should be equal parts thrilled and humbled by the prospect of transforming a beloved fantasy book into something that can grace screens the world over.
Link to the rest at The Bookseller
PG says this trend is all the more reason for authors to hold on to their subsidiary rights or, if traditionally-published, bump the royalty rates up for subrights or negotiate for an increasing percentage of subsidiary rights as gross income to the publisher from subrights hits certain revenue levels.
Most books, indie or traditional, aren’t adapted for motion pictures or televisions, but if lightning strikes with a big subrights deal, it will almost certainly because the author did a great job of writing the book instead of the publisher doing better than usual in selling print and ebook rights.
Book Sales Up, Readership Down
From The Authors Guild:
Both publishers and booksellers celebrated the news that print book sales were up 9.1 percent last year. According to Publishers Weekly, booksellers sold 825.7 million books in 2021, up from 757.9 million in 2020. A huge increase in fiction units sold led the way, with young adult fiction sales jumping 30.7 percent, adult fiction up 25.5 percent, and children’s fiction up 9.6 percent, respectively. All told, print book sales have risen more than 18 percent since the start of the pandemic in early 2020.
U.S. Readership Lowest in Two Decades
The statistics on female readership are specifically troubling. For decades, women read nearly twice as many books as men, but the gap has narrowed significantly. The average American woman read 15.7 books last year compared to 19.3 books five years ago. While male readership declined only slightly over the same time period, going from 10.4 books in 2016 to 9.5 in 2021, this decrease in the number of books women read will particularly impact fiction sales, given that women account for 80 percent of all fiction sales in the U.S., U.K., and Canada.
The overall decline in readership is likely due to increased interest in other at-home leisure activities, particularly digital streaming services. Just six percent claimed reading to be their favorite way to spend an evening, far below spending time with family (33%) or watching television or movies (23%). Gallup notes that this is only the second time since 1960 that less than 10 percent of Americans didn’t select reading as their top favorite evening activity.
. . . .
Paper Shortages Continue to Delay Book Publication
“Paper mills are not only cutting back, but they’re switching from book grade papers to, in their view, more profitable types of paper products,” said Integrated Books International’s Bill Clockel in a recent interview. “So even though some mills might have closed, more likely than not they’re not making book papers anymore. That’s the biggest problem that we see. There are other challenges with obtaining consumables, but paper clearly is the biggest one.”
Labor also remains an issue due to worker shortages attributable to both COVID-19 and increased employee turnover, as the quit rate among warehousing workers, which includes book distribution centers, ranked the third highest in the nation in November 2021 according to the U.S. Bureau of Labor Statistics.
Cautious Optimism
Though the majority of U.S. authors have experienced significant income declines since the start of the pandemic, many in the book industry remain positive. The percentage of Americans reading e-books rose five percent in the past two years
Link to the rest at The Authors Guild
PG will reveal that during the same period of time discussed in the OP, the earnings of many indie authors, including Mrs. PG, from Kindle Direct Publishing have been climbing.
Hitler’s American Gamble
From The Wall Street Journal:
Most Americans, if asked, would probably say that Franklin Roosevelt declared war on Nazi Germany, following the bombing of Pearl Harbor on Dec. 7, 1941. Since we were at war with imperial Japan, the logic would run, we were obliged to be at war with Japan’s Axis ally.
In fact, it was Adolf Hitler who declared war on the United States—four days after Pearl Harbor, on Dec. 11, 1941. By doing so, he managed to bring the full weight of America’s industrial might against him. The war declaration ranks as Hitler’s worst strategic blunder—even worse than his decision to invade the Soviet Union in June 1941, when he pitted the Wehrmacht against an opponent with much greater manpower reserves and strategic depth.
In “Hitler’s American Gamble,” Brendan Simms and Charlie Laderman—historians at the University of Cambridge and King’s College, London, respectively—provide an engaging and insightful account of the forces that shaped Hitler’s fateful decision. The authors note that, far from being an irrational or impulsive gesture, Hitler’s war on America “was a deliberate gamble.” It was driven, in part, by “his geopolitical calculations” and “his assessment of the balance of manpower and matériel.” The decision derived as well, the authors assert, from Hitler’s tortured view of the relations among Britain, the U.S., and, not least, the Jews in both Europe and America.
On the eve of Pearl Harbor, Hitler was heavily engaged in waging war on Britain, and he seemed close to winning. Yet he was hesitant to deliver the knock-out blow. He had already missed an opportunity to do so in the spring of 1941, when Britain evacuated Greece and Crete and Rommel’s Afrika Korps was scoring success after success against British forces in North Africa. Hitler believed that his real enemy was Winston Churchill, not the British people, and that the British people would eventually give up the fight and accept Nazi hegemony in Europe. At the same time, he was well aware that it was the U.S. and its supplies of food and war matériel—sent across the Atlantic under the terms of Lend-Lease—that were keeping Britain in the fight.
In Hitler’s mind, then, America was a grave threat to his plans for German hegemony—indeed, Germany was locked in deadly combat with “the Anglo-Saxon powers,” Britain and the United States. But that is not all. Hitler believed that, as Messrs. Simms and Laderman put it, “ ‘the Jews’ had manipulated the ‘Anglo-Saxons’ into war with the racially kindred Reich.” Race-paranoia was a critical component of Hitler’s “gamble.”
Hitler was convinced that Japan’s surprise attack would divert U.S. resources and attention just long enough to secure Britain’s isolation and surrender. And the German panzer divisions poised only 12 miles from Moscow signaled the imminent collapse of his only other opponent, Russia. In the event, he was wrong on both counts. What was about to collapse in Russia wasn’t the Red Army but the Wehrmacht, as Hitler’s panzers were thrown back from Moscow and nearly half a million German soldiers perished in the winter of 1941-42. Meanwhile, Japan’s victories in the aftermath of Pearl Harbor proved to be too brittle to last.
Link to the rest at The Wall Street Journal (Should be a free link, but if it stops working, PG apologizes for the paywall.
The Benefits of Writer Friends
From Publishers Weekly:
I’ve never been particularly great at making friends. As a woman with both ADHD and autism, small talk is hard, and reading social cues is even harder. I tend to either overshare or clam up entirely, and both have led to plenty of awkward moments that felt mortifying at the time but give me a good laugh when I look back at them. Adolescence was challenging, and masking my neurodivergence always left me exhausted, but taking off that mask and embracing neurodivergent info dumping about special interests and my directness with my peers often left me on the outskirts of social circles. My best friends in middle and high school were the characters in the books I devoured.
. . . .
I wrote, queried, and went on submission with my debut novel, A Brush with Love, without knowing anyone else who had endured the process—who could share useful strategies or advise what to expect and what questions to ask. Navigating the emotional roller coaster of the process without someone to commiserate with was tough.
As authors, our careers are steeped in vulnerability. We must be soft enough to create yet tough enough to take criticism, and then brave enough to try again. It’s an isolating journey, and one I was quickly feeling burned out from without any writer friends to lean on.
But I didn’t know where to start with finding them. I think a part of me—the awkward tween who never quite fit in anywhere—had clutched on to the hope that friends would find me, that I could be a passive bystander in developing the friendships I so greatly craved.
. . . .
So, one day, with a glass of wine providing liquid courage and absolutely zero couth, I made it a mission to actually do something to make a friend. It was as simple, albeit terrifying, as telling an author how much I loved their work and that I’d like to be their friend if they were open to it.
Can you believe that actually worked?! Because sometimes I can’t. I had no idea being direct and honest—something that had so often made me a weirdo among my peers—could allow me to form some of the most fulfilling friendships I’ve ever had.
By being vulnerable and getting out of my own way, I’ve found that other writers are also looking for that connection. We spend weeks, months, years pouring our souls into our pages, holding our hearts in the tips of our fingertips as we craft our characters and story only to rework it, restructure it, experience the highs of it being loved, and the crushing lows of it being torn apart. Being able to share all those feelings with someone who gets it—really gets it—has both taught me skills and brought me unexpected joy.
The most important aspect of cultivating these bonds is making friends simply for the joy of the relationship, not for what transactional benefit someone else can provide. One doesn’t need an endless stream of bestselling authors texting them or tweeting about their work to make the publishing experience meaningful. I’ve learned that opening up and being vulnerable with others can create a safe space for everyone to be their truest self. And that’s where the real fun begins. Whether it’s a single person or an entire group, finding friends in the chaos of publishing carries with it endless opportunities to laugh, to cry, to cheer someone’s big wins or show solidarity in the group chat when someone experiences anxiety or disappointment.
Link to the rest at Publishers Weekly